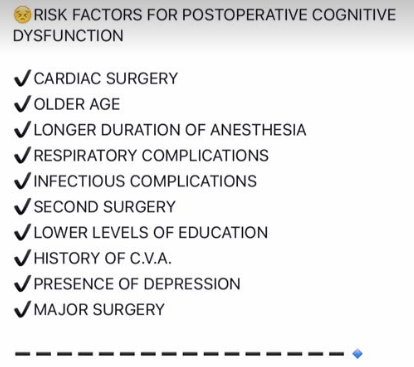
POSTOPERATIVE COGNITIVE DYSFUNCTION – RISK FACTORS
Incidence up to more than 40%
Might be occurring together with EEG-changes
Methods usually tried to reduce the incidence: addition of nitrous oxide, premedication with benzodiazepines, early extubation, switching to other inhaled anaesthetics
Propofol maintenance after sevoflurane induction seems to be the best alternative.
A recent study also indicates that a switch to desflurane for maintenance after sevoflurane inhalation induction reduces the incidence of emergence agitation by 50 %
A paranoid delusion is said to be a common feature of this state of agitation.
Information about this phenomenon should be explained to the parents before the procedure.
1. The evaluation of risk factors, is for planning the anesthetic management, and will be of no use in predicting the outcome.
2. There is no justification for performing revascularisation purely to facilitate elective non cardiac surgery.
3. M.I. within the last 6 weeks, class iii-iv angina, decompensated heart failure, malignant arrhythmias, severe valvular heart disease, CABG/PTCA within the last 6 weeks constitute major Cardio Vascular risk factors for surgery.
4. Previous M.I. (>6weeks), class i-ii angina, compensated heart failure, T2 DM constitute intermediate C. V. risk factors.
5. Age > 70 years, uncontrolled systemic hypertension, arrhythmias, family h/o CAD, dyslipidemia, smoking, renal dysfunction, ECG abnormalities (LVH, RBBB/LBBB, ST segment anomalies) constitute minor C. V. risk factors.
6. Only emergency, life saving procedures should be performed during the first 6 weeks after a myocardial infarction (M. I.) and after CABG/PTCA with or without a coronary stent. The period between 6 weeks and 3 months are considered as a period of intermediate risk, when non urgent elective surgery should be postponed.
7. SURGICAL PREDICTORS OF INCREASED PERIOPERATIVE CARDIOVASCULAR RISK
(i) HIGH RISK (complication rate >5%)
#Emergency major to intermediate surgery, especially in elderly patients
#Aortic & major vascular surgery; and also peripheral vascular surgery
#Procedures involving: hemodynamic instability, long duration or large fluid/blood loss
(ii) INTERMEDIATE RISK (complication rate 1-5%)
#Carotid endarterectomy
#Head & neck surgery
#Abdominal/thoracic surgery
#Orthopaedic surgery
#Prostatectomy
(iii)LOW RISK (complication rate <1%)
#Endoscopic procedure
#Breast and superficial surgery
#Eye surgery
8. ACE inhibitors are withheld for 24 hours by some anesthetists.
9. Perioperative beta blockade should be continued for 72 hours postoperatively.
10. The gold standard for detecting intraoperative ischemia and assessing volume status & valvular function is TEE.
11. Most perioperative myocardial infarctions occur in the first 3 days postoperatively. Patients at risk for M.I. require effective analgesia and humidified oxygen therapy for atleast 72 hours after major surgery.
12. Severe hypertension (grade 3) has been associated with an increased incidence of perioperative hemodynamic instability, silent m.i. and arrhythmias; but evidence of a clinically significant increase in adverse outcome is lacking. The presence of endorgan damage due to hypertension is more important than the blood pressure per se.
13. Ideally the blood pressure should be maintained within 20% of the best estimate of preoperative pressure.
14. The treatment of arrhythmias produced by WPW syndrome includes Flecainide, Disopyramide, Procainamide and Amiodarone. Digoxin and Verapamil are contraindicated.
15. There is no evidence to suggest that, frequent ventricular ectopics or asymptomatic non sustained ventricuar tachycardia is associated with an increased incidence of perioperative M.I.
16. Sick sinus syndrome is associated with a high risk of thromboemboism and may be anticoaguated. If the patient is not having a permanent pacemaker, he/she needs a, temporary pacing wire inserted preoperatively.
17. Complete heart block, type ii second degree A-V block and lesser degrees of heart block, in the presence of symptoms or cardiac failure requires preoperative insertion of permanent or temporary insertion of pacemaker. Volatile agents prolong cardiac conduction and can worsen heart block. Atropine, Isoprenaline and facilities for external pacing should be kept ready.
18. ATRIOVENTRICULAR BLOCKS
(i) First degree block: P-R interval > 0.2 sec
(ii)Second degree block
Type I: progressive lengthening of PR interval, until conduction fails and a beat is dropped.
Type II: intermittent failure of AV conduction without preceding PR prolongation.
(iii) Third degree block
Complete dissociation of atria and ventricles as atrial impulses fails to be transmitted.
19. CHECKLIST FOR A PATIENT WITH PACEMAKER
a. Indication for pacemaker insertion
b. Mode of function of pacemaker
c. Functional status
d. Consider conversion of rate responsive pacemakers to fixed rate in the perioperative period.
e. Ensure use of only bipolar diathermy
f. If unipolar diathermy must be used, then the ground plate should be placed on the same site as the operating site, as far away from the pacemaker as possible. The frequency and duration of use should be minimised and the lowest possible current used.
g. MRI is contraindicated
h. Magnets should not be placed over pacemakers during surgery, as they have an unpredictable effect on the programming of modern pacemakers.
i. A backup pacing system, atropine, adrenaline, isoprenaline and a backup pacing system should be available, in case of pacemaker failure.
20. Anesthesia constitutes a significant risk in Hypertrophic Obstructive Cardiomyopathy. Patients will be having dynamic left ventricular outflow tract obstruction, often with secondary MR. They are prone to arrhythmias and sudden cardiac death. Look for an Ejection systolic murmur in auscultation and LVH in ecg. Confirmation is by ECHO. Avoid hypovolemia, vasodilatation and the use of catecholamines
21. Constrictive pericarditis poorly tolerate vasodilatation; especially at induction.
22. In valvular heart disease, antibiotic prophylaxis is especially required for dental surgeries and those involving instrumentation of upper respiratory tract and genitourinary system.
23. AORTIC STENOSIS
# Even an ejection systolic murmur in an asymptomatic patient also warrants careful preoperative examination/ ECHO, as symptoms tend to appear late in the disease only.
# Promptly treat tachycardia and AF.
# Maintain ventricular filling by avoiding hypovolemia and maintaining SVR.
# Vasodilatation may result in profound hypotension–> subendocardial ischemia and even sudden death.
# Aggressive treatment of hypotension is mandatory to prevent cardiogenic shock and/or cardiac arrest. Cardiopulmonary resuscitation is unlikely to be effective in patients with aortic stenosis because it is difficult, if not impossible, to create an adequate stroke volume across a stenotic aortic valve with cardiac compression.
24. AORTIC REGURGITATION
# Avoid vasoconstriction and bradycardia which increases the degree of regurgitation
# A mild tachycardia, moderate fluid loading, a degree of vasodilatation and avoidence of myocardial depression can improve the forward flow.
# Acute AR is a surgical emergency and may respond poorly to vasodilatation.
25. MITRAL STENOSIS
# Patients are prone to develop CCF and Pulmonary Edema.
# Atrial fibrillation is a trigger for acute deterioration; so should be treated preoperatively
# Avoid tachycardia, myocardial depression and excessive vasodilatation
# Hypovolemia compromises ventricular filling
# Fluid overload can easily precipitate pulmonary edema
# PCWP will be inaccurate in the presence of pulmonary hyperension. Avoid Nitrous oxide if there is evidence of pulmonary hypertension.
26. MITRAL REGURGITATION
# A mild tachycardia, a slight reduction in SVR and avoidance of myocardial depression are desirable.
# Avoid hypovolemia
27. There is little evidence that GA in ADULTS with URTI is associated with an increased risk of adverse respiratory events, although upper airway reactivity may be increased
28. In children with URTI, a higher incidence of adverse respiratory events have been demonstrated, but few of these adverse events result in postoperative sequelae. It has been suggested that surgery need not necessarily be postponed in children with mild URTI. Increased airway reactivity may persist for 4-6 weeks and if surgery is postponed, it should be for a period of at least 6 weeks.
29. In COPD, if the patient is having copious secretions, better to avoid anticholinergics, as it will impair the ability to clear secretions.
30. Even though regional anesthesia has the advantage of avoiding respiratory complications of GA, most patients, even those with quite severe COPD may be managed safely under carefully conducted GA.
31. Pressure Controlled Ventilation with a low respiratory rate and prolonged expiratory phase is suitable in COPD patients.
32. Epidural analgesia has been shown to decrease the incidence of postoperative pulmonary complications in thoracic and upper abdomnal surgery.
33. In patients with bronchial asthma, good depth of anesthesia, good muscle relaxation and i. v. Lidocaine can reduce the incidence of bronchospasm during intubation; topical lidocaine spray is not effective and may induce bronchoconstriction in some patients.
34. Circulatory disturbance during anesthesia and surgery may affect the absorption of subcutaneous insulin.
Follow up the patient:
If voice is not improving: (Better to call the ENT Surgeon to do this-) Do a laryngoscopy and using any instrument, just give a mild pressure on aretynoid; usually it will fall back to correct position.
If speech is improving, advice VOCAL CORD ADDUCTION EXERCISES
Standing position.. Take a deep inspiration
and stop..and hold the breath.. this closes glottis..now strongly fall over and push against a wall…keep it for a few seconds.. Repeat this a few times.. This can force the aretynoid back to normal position by a stretching force… Usually voice is regained by this after 2 days..
Or lift heavy weights after deep inspiration (not for CAD patients)
Plus continue Speech Therapy
Problem occurs, when Aretynoid dislocates, and nobody attempts to relocate it, and it get fixed in that position..
1.Hypothyroidism
2.Anemia
3.Reduced plasma volume
4.Impaired hepatic drug metabolism
5.Hypoglycemia
6.Impaired clearance of free water
7.Hyponatremia
8.Enlarged tongue
9.Nerve compression due to myxoedema
10.Delayed gastric emptying
# NPPO is associated with upper airway obstruction in a spontaneously breathing patient.
# It occurs in 0.05–0.1% of all general anaesthetic cases and laryngospasm has been reported as being the cause in 50% of cases.
#The clinical course is most frequently observed on emergence from anaesthesia where incomplete recovery from general anaesthesia increases the likelihood of the development of laryngospasm, but it has also been reported after airway obstruction with a foreign body and blockage and biting of tracheal tubes, hanging, and strangulation.
#Pulmonary oedema is typically described as developing within 2 min of the obstruction.
Once the airway is occluded, the spontaneously breathing patient will continue to generate negative intrathoracic pressure which will increase substantially as respiratory distress develops.
#There is an associated increase in sympathetic tone due to the stress of hypoxia and airway obstruction which increases SVR and elevates pulmonary artery pressure.
This is further exacerbated by hypoxic pulmonary vasoconstriction.
#The combination of these processes creates a pressure gradient across the capillary–alveolar membrane which favours the movement of fluid into the lung parenchyma.
#It is most common in younger patients, presumably because they are able to generate higher negative inspiratory pressures and, arguably, have a higher sympathetic tone and better cardiac function.
#The condition may resolve rapidly after definitive management of the airway obstruction, but in some cases, copious pulmonary oedema may form and it can be associated with pulmonary haemorrhage suggesting capillary membrane damage.
#After recognition of the cause of obstruction, the treatment required ranges from relatively modest support such as brief periods of CPAP for 2 h to positive pressure ventilation over a period of 24 h.#TheLayMedicalMan
Ref: Neurogenic pulmonary edema, Ronan O’Leary, Justin McKinlay, Contin Educ Anaesth Crit Care Pain (2011) 11 (3): 87-92.
http://feeds.feedburner.com/TheLayMedicalMan
🔸In the pregnant patient, the respiratory function deviates from the normal
🔸There is increased CO2 production by the mother and the foetus; but mostly you see a respiratory alkalosis. Why?
🔸This is because the stimuli from the raised pCO2 levels and that by the respiratory stimulant, progesterone, sets the minute ventilation approximately 30% higher than the normal levels and this is more than what is needed to compensate for the increased CO2 production
🔸It is mainly the reduction in FRC (a reduction by 10-25% ; appears by 12th week ; is due to the reduced chest wall compliance ; lung compliance is normal ) which makes the patient more vulnerable to hypoxia.
🔸The alveolar diffusing capacity is reported to be normal during pregnancy
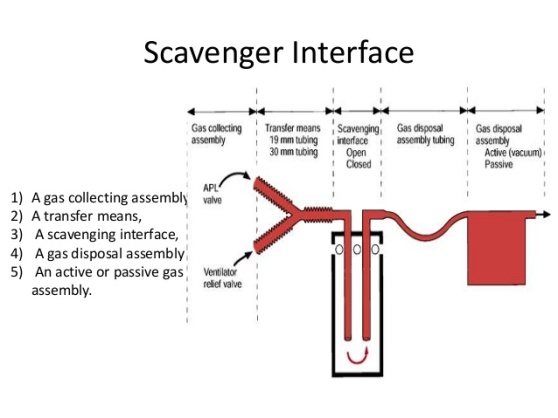 Scavenging refers to the method of extracting waste gases from the breathing system and venting them to an area where they will not be directly inhaled by staff or other patients.
Scavenging refers to the method of extracting waste gases from the breathing system and venting them to an area where they will not be directly inhaled by staff or other patients.📌Ictal bradycardia/asystole is a poorly recognised cause of collapse late in the course of a typical complex partial seizure
📌It is important to identify ictal bradycardia as a potential harbinger of lethal rhythms, such as asystole, as this may be one important mechanism leading to sudden unexpected death in epilepsy (SUDEP)
📌Tachycardia is the most common rhythm abnormality occurring in 64–100% of temporal lobe seizures. Ictal bradycardia has been reported in less than 6% of patients with complex partial seizures
📌The ictal bradycardia syndrome occurs in mostly in patients with temporal lobe seizures.
📌It is believed that abnormal neuronal activity during a seizure can affect central autonomic regulatory centres in the brain leading to cardiac rhythm changes.
📌Ictal bradycardia/asystole may be unrecognised until documented during video-electroencephalograph (video EEG)–electrocardiogram (ECG) monitoring in those with refractory epilepsy, often in the context of pre-surgical evaluation
📌Other rhythm abnormalities which can occur are change in heart rate variability, ictal tachycardias and atrioventricular (AV) block
📌If sufficiently severe, the ictal-induced bradyarrhythmia temporarily impairs both cerebral perfusion and cortical function; the result has the dual effect of terminating the seizure, while at the same time triggering syncope with consequent loss of consciousness and postural tone. In essence, a complex partial seizure patient may manifest both seizure and syncope features during the same episode.
📌There are currently no guidelines on who should undergo further cardiovascular investigations ; dual chamber pacemaker implantation has been suggested as a treatment in the long term, for epilepsy patients who manifest this syndrome and suffer repeated falls; but there is not much mention in literature both about diagnosis and about pharmacological and non pharmacological interventions to counter such episodes when presenting as an emergency situation in the perioperative scenario , especially when the patient is under anesthesia.
#Neurology , #NeuroCriticalCare , #Anesthesia , #LayMedicalMan , #CriticalCare , #Epilepsy , #Cardiology , #CardiacAnesthesia
Reference: Ictal bradycardia and atrioventricular block: a cardiac manifestation of epilepsy; Salman S. Allana Hanna N. Ahmed Keval Shah Annie F. Kelly, Oxford Medical Case Reports, British Journal of Cardiology : Ictal Bradycardia and Asystole Associated with Intractable Epilepsy: A Case Series Elijah Chaila, Jaspreet Bhangu, Sandya Tirupathi, Norman Delanty; Ictal Asystole-Life-Threatening Vagal Storm or a Benign Seizure Self-Termination Mechanism? David G. Benditt, Gert van Dijk, Roland D. Thijs (Editorial:Circulation )
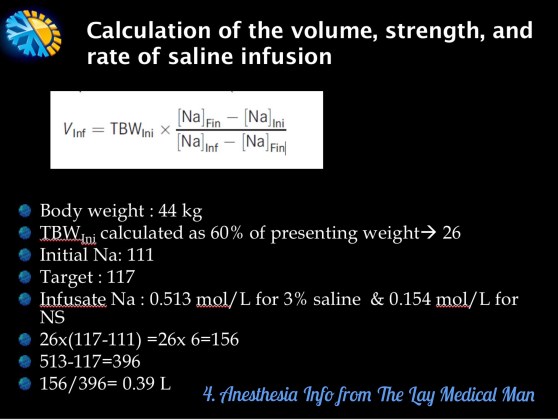
🚩#TURPsyndrome is diagnosed based on clinical signs, symptoms and biochemical findings
🚩The manifestations are due to hypervolemia, hyponatremia and due to the direct toxicity of the irrigation fluids like 1.5% glycine
▪️FACTORS INCREASING THE ABSORPTION OF THE IRRIGATION FLUID ( AND THUS CONTRIBUTING TO THE HYPERVOLEMIA )
🚩Long duration of the surgery: the irrigation fluid is absorbed at the rate of 20-30 mL/ min and so the volume absorbed increases with the duration of the surgery
🚩High pressure delivery of the irrigation fluid especially from a considerable height; the minimum height required for adequate flow should be used (usually 70 cms)
🚩Low venous pressures
🚩Excessive bleeding (= there are more open veins)
🚩Large prostate (>50g)
▪️CLINICAL FEATURES:
🚩Headache, Restlessness, Agitation, Confusion, Convulsions, Coma; pulmonary oedema may also set in. If patient is under general anesthesia, these symptoms will get masked.
▪️MANAGEMENT FROM SURGICAL SIDE:
🚩Coagulating bleeding points and terminating surgery as soon as possible.
▪️ANESTHETIC MANAGEMENT:
🚩Reduce / stop fluid administration. Diuretics may be required in the presence of pulmonary oedema
🚩Intubation to protect the airway and mechanical ventilation to support respiration may be required
🚩Anti-convulsants, if needed, to treat seizures
🚩Hypertonic saline should be considered for severe hyponatremia (<120 mmol L−1) or in the presence of severe neurological symptoms.
👉🏿N.B.- Central pontine myelinolysis or osmotic demyelinating syndrome (ODS) is more likely to occur with correction of serum Na greater than 8-12 mmol/day and in the setting of chronic hyponatremia (greater than 48 h)
👉🏿Faster rates of administration can potentially lead to central pontine myelinolysis. Treatment should stop once symptoms have resolved or the serum sodium is more than 125 mmol L−1. Such therapy is best delivered in a high-dependency environment.
🔻A template is given below for calculating the volume of hypertonic saline
#anesthesia , #urology ,#hyponatremia , #anaesthesiologist