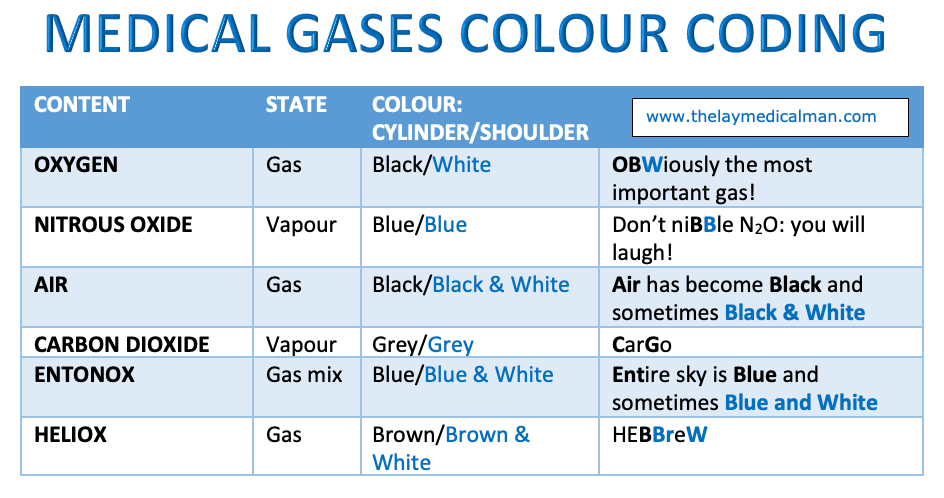
MEDICAL GASES: COLOUR CODING
The flowmeter / rotameter is a variable-orifice device used to measure the flow of oxygen, air and nitrous oxide in the anesthesia machine
It usually contains a bobbin
The pressure of gas beneath the bobbin pushes it up the flowmeter until the force beneath it is balanced by the force of gravity pulling it back to its resting position.
The variable orifice of the flowmeter means that the flow of gas past the bobbin at low flows is laminar, but at high flows it is turbulent.
The flutes on the bobbin are to ensure continuous movement of the bobbin as gas passes it, showing that it is not stuck.
The variable orifice of the flowmeter is responsible for the turbulent flow.
Impedance is a term that is commonly used in the world of #electrophysiology and #BiomechanicalEngineering.
The chance of getting an electric shock is high when you have wet hands because the impedance of the skin is lower than when it is dry.
Thoracic impedance increases during inspiration.
When applying electric current to the chest during #defibrillation, less energy may reach the heart during the inspiratory phase than during the expiratory phase because of this phenomenon, thereby decreasing the possible success of defibrillation.
So better to attempt defibrillation during the expiratory phase of mechanical ventilation.
Where the #resistance of a circuit is dependent on the frequency of the current through it, the term impedance is used.
The unit of impedance is therefore the same as that of resistance (the ohm), but the symbol Z is used to differentiate it from the symbol used for resistance (Ω).
In case of a capacitor, as the frequency of the current increases, the current passes through the circuit more easily, i.e. the resistance of the capacitor falls with increasing current frequency.
In contrast, the resistance of an inductor rises as the frequency of the current increases.
#PhysicsForAnesthesiologist , #anesthesiologist , #anesthesia , #biomedical
Davis PD, Kenny GNC. Basic Physics and Measurement in Anaesthesia, 5th edn. Oxford: Butterworth–Heinemann, 2003; pp. 149–64 . Ewy GA, Hellman DA, McClung S, Taren D. Influence of ventilation phase on transthoracic impedance and defibrillation effectiveness. Crit Care Med 1980; 8: 164–6
Entonox is Nitrous oxide mixed 50:50 with oxygen
It provides analgesia with maintenance of consciousness.
Usually administered via a demand valve for self administration.
Takes 30 seconds to act and continues for approx. 60 sec after inhalation has stopped
For optimum effect inhalation should start when the contraction tightens. This will co-ordinate the maximal effect with the central painful part of the contraction.
20% N20 is equivalent to 15 mg of subcutaneous morphine.
The optimal analgesic concentration was found to be 70% but some mothers lost consciousness at this concentration
50% N20 in oxygen is safer and this has become standard now
Entonox is the BOC trade name for this gas mixture.
Poynting effect
The Poynting effect involves the dissolution of gaseous O2 when bubbled through liquid N2O, with vaporisation of the liquid to form a gaseous O2/N2O mixture.
Critical & Pseudocritical temperature
The critical temperature of a gas is the maximum temperature at which compression can cause liquefaction. Or it is the temperature above which a substance cannot be liquefied however much pressure is applied. Mixing gases may change their critical temperature.
The pseudocritical temperature applies to a mixture of gases, such as Entonox, and is the temperature at which gas mixtures separate into their component parts.
The Poynting effect produces a 50:50 mixture which reduces the crtical temperature of N20 so Entonox has a pseudocritical temperature of -6 degree.
Entonox
Highest -5.5°C @117 bar
Cylinder -7°C @137 bar
Pipeline -30°C @4 bar
In cylinders it is supplied at a pressure of 137 bar and must be stored above its pseudocritical temperature of -6°C.
Below this temperature the N2O liquefies in a process called lamination. If this occurs a high concentration of O2 will be delivered first with little analgesic effect, but as the cylinder empties the mixture will become progressively more potent and hypoxic as it approaches 100% N2O.
If a cylinder has been exposed to cold below -6 degree C it should be warmed for 5 minutes in a 37 degree C water bath or for 2 hours in a room at 15 degree C. It should then be inverted three times before use.
When delivered via a pipeline at 4.1 bar the pseudocritical temperature is less than -30°C.
Altitude per se has no effect on Entonox.
Reference: www.frca.uk
Dynamic or absolute viscosity is a measure of the resistance of a fluid or gas to flow. It is measured using a viscometer or rheometer.
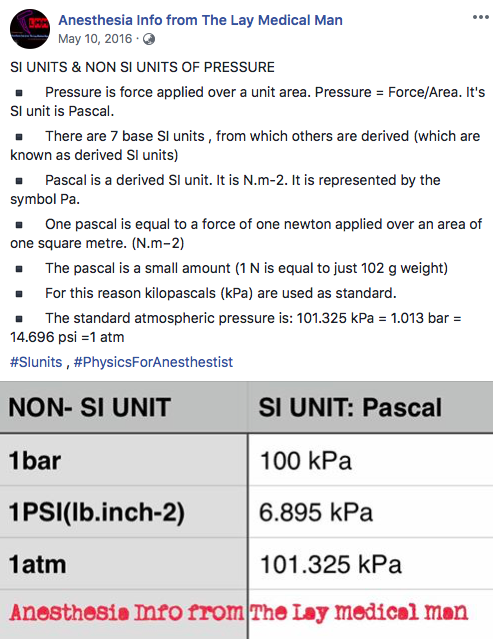
The SI unit of dynamic (or absolute) viscosity is the pascal-second (Pa·s), equivalent to N·s/ m2.
Viscosity is independent of flow rate
Viscosity is independent of pressure
For a gas, viscosity decreases as its temperature increases
The relationship between viscosity and temperature and pressure only holds true for those fluids and gases that exhibit ‘Newtonian’ properties, i.e. substances that will always flow irrespective of forces acting upon them (e.g. crystalloid solutions and water).
Blood is a non-Newtonian fluid and its viscosity depends largely on haematocrit (and varies with flow rate).
Blood viscosity is increased by volatile anaesthetic agents, smoking and aging
A thixotropic substance is one that becomes less viscous over time when agitated. If it becomes more viscous with agitation, this is known as a rheopectic material.
Kinematic velocity is defined as the dynamic velocity of a substance divided by its density.
For this, we should know:
1. Oxygen delivered = FiO2 x Minute Volume
2. Duration of the transfer
For e.g. If we are expecting a duration of 2 hours (120 minutes) and we are having Size E cylinders and also need to deliver an FiO2 of 1 @ 6L / min
1. O2 delivered = 1 x 6 = 6L/ min
2. Size E has 660 L of O2, which will suffice for 660/6= 110 minutes ; so for 120 minutes, we need 2 cylinders
