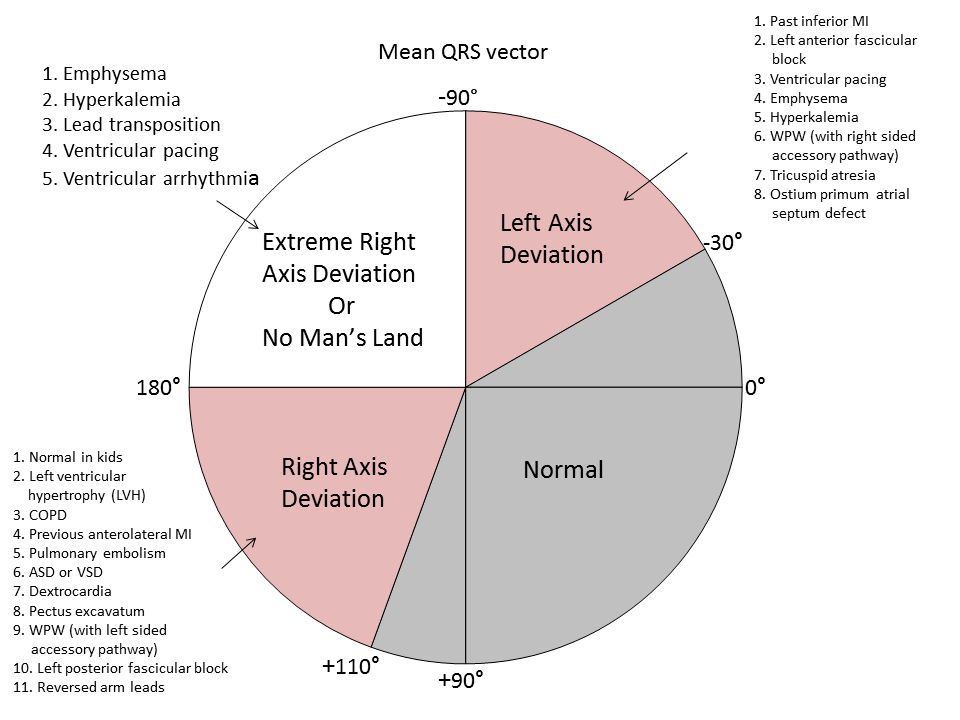
ECG AND AXIS
TEG is a relatively new modality for monitoring coagulation which is very useful during management of trauma and also in the perioperative scenario..
BASIS:
INTERPRETATION
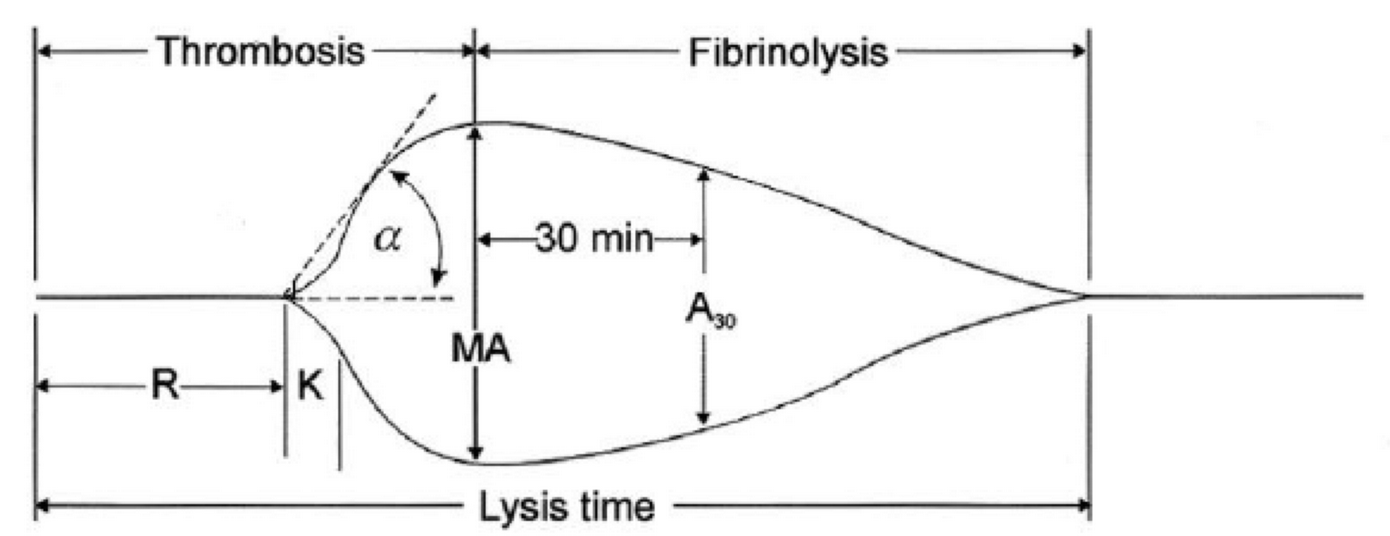
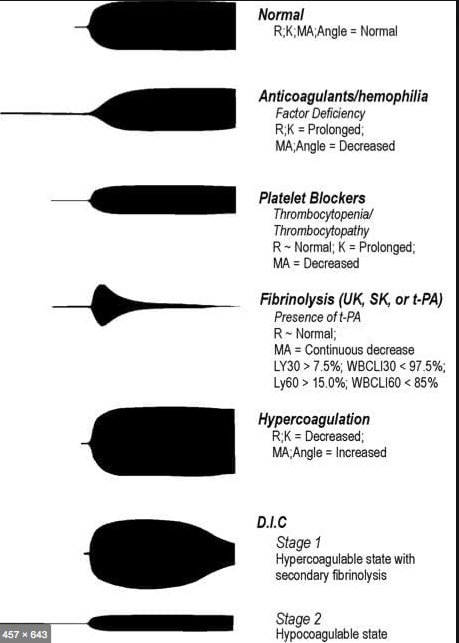
R(sec): The first measurement of note is the reaction time (R time). This is the time interval from the start of the test to the initial detection of the clot. Normal R values range between 7.5 and 15 minutes. A prolonged R time may indicate hemodilution or clotting factor deficiencies. The treatment for prolonged R time is to administer FFP as it contains all factors of the coagulation cascade, without further coagulant hemodilution. A shortening of R time (< 3 minutes) occurs in hypercoagulable states. Examples would be patients with early disseminated intravascular coagulation (DIC) or septicemia. In these situations, free thrombin is released into the circulating blood, triggering the clotting mechanisms but the patient later begins to bleed because of exhaustion of clotting factors.
K (sec) and Angle α (°): The clot strength is measured by these 2 variables in TEG. The K value measures the interval between the R time and the time when the clot reaches 20 mm. Normal K values range between 3 and 6 minutes. Prolongation of the K value with normal platelet count indicates inadequate amounts of fibrinogen to form fibrin. The treatment for prolonged K value is therefore to administer fibrinogen/cryoprecipitate. The α angle measures a line tangent to the slope of the curve during clot formation.The alpha angle represents the thrombin burst and conversion of fibrinogen to fibrin. Normal α value is between 45° and 55°. A longer K value causes a shallow or more acute angle (<45°), while a shorter K value causes a steeper α angle (>45 °). An angle α <45° suggests a less vigorous association of fibrin with platelets. In this case, treatment begins much higher on the coagulation cascade, with the replacement of both fibrinogen and factor VIII. Thus, these patients can be treated with the administration of cryoprecipitate. Shortening of the K-value indicates a very quick formation of clot, potentially due to hypercoagulability or inappropriate consumption of coagulation factors. A shortened K value also corresponds to a steeper α (>45°). The treatment for shortened K and steeper α is anticoagulation therapy
Ref: Thromboelastography: Clinical Application, Interpretation, and Transfusion Management, Shawn Collins et al AANA Journal Course, 2016
HOW DO WE TEST CLOTTING?
Normal value is 3 to 10 minutes.
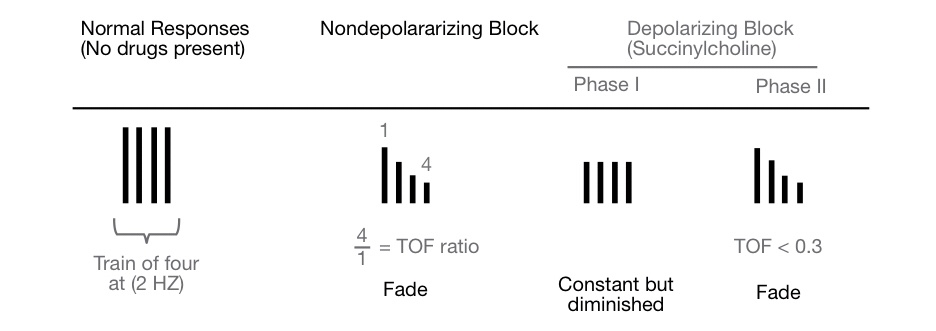
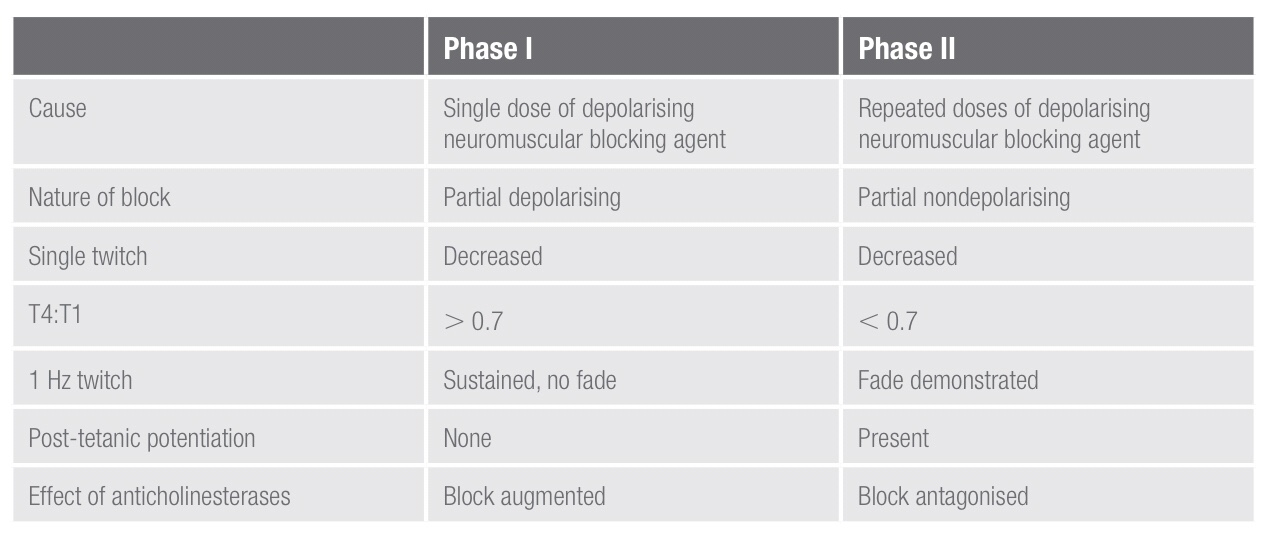
• Reduced twitch height, but sustained response to tetanic stimulation
• No post-tetanic facilitation; does not exhibit fade during tetanus or train-of-four
• TOF ratio >70% (height of fourth twitch to that of first). This is a measure of the pre-synaptic effect of suxamethonium.
The block is potentiated by the effect of anticholinesterases because these
will further decrease the rate of suxamethonium breakdown.
A phase II block describes the block seen following the repeated administration/infusion of suxamethonium and can develop with doses
in excess of 2.5 mg/kg. It occurs because in the continued presence
of suxamethonium, the receptors eventually close and the membrane
repolarises, at least partially. However, it is now desensitised to ACh and so
cannot open again to propagate an action potentials. In this way, a phase II
block is similar to a non-depolarising block. Phase ii blocks are also called
‘desensitisation blocks’.
characteristics of a phase ii block:
• Exhibits fade on tetanic stimulation
• Exhibits post-tetanic facilitation
• TOF ratio < 0.3 (fourth to first twitch height)
• Antagonised by anticholinesterases
• Tachyphylaxis is seen with the need to increase suxamethonium infusion
rate or bolus dose.
What’s the problem, if we place the temperature probe in upper 1/3rd or 2/3rd of the esophagus?
Esophageal temperature should be taken from the lower third of the oesophagus; placed above this level, the probe may under-read due to cooling effect of inspired gases. It gives a good estimate of cerebral blood temperature.
What’s the advantage of nasopharyngeal temperature measurement over oesophageal measurement?
The nasopharyngeal temperature probe is placed just behind the soft palate. The advantage is that it is more accessible compared to the oesophageal temperature measurement. The disadvantage is that it is less accurate in representating the core temperature.
What are the advantages of measurement of temperature @ Tympanic membrane?
The tympanic membrane provides an accurate representation of hypothalamic temperature. It is less invasive, has a short response time and correlates well with oesophageal temperature. But it does not allow continuous measurements.
What is the best method for CONTINUOUS measurement of core temperature?
Blood temperature measurement using a pulmonary artery flotation catheter
What are the factors reducing the accuracy of Rectal temperature measurement?
Rectal temperature is influenced by heat generated from gut flora, the cooling effect of blood returning from the lower limbs and the insulation of the probe by faeces. It is normally about 0.5–1.0 ° C higher than core temperature and has a slow response time.
Can you say an e.g. of utilising the temperature gradients existing between different sites of the body for clinical advantage?
The gradient between a skin temperature and a core temperature can be used as a marker of peripheral perfusion.


TOF response %of receptors occupied
0 —————–100
1 ——————95
2—————— 90
3 ——————85
4 —————-<75
🔸In the pregnant patient, the respiratory function deviates from the normal
🔸There is increased CO2 production by the mother and the foetus; but mostly you see a respiratory alkalosis. Why?
🔸This is because the stimuli from the raised pCO2 levels and that by the respiratory stimulant, progesterone, sets the minute ventilation approximately 30% higher than the normal levels and this is more than what is needed to compensate for the increased CO2 production
🔸It is mainly the reduction in FRC (a reduction by 10-25% ; appears by 12th week ; is due to the reduced chest wall compliance ; lung compliance is normal ) which makes the patient more vulnerable to hypoxia.
🔸The alveolar diffusing capacity is reported to be normal during pregnancy
SSEP reflect the ability of a specific neural pathway to conduct an electrical signal from the periphery to the cerebral cortex.
👉🏿THIS IS WHAT WE DO:
A skin surface electrode is placed near a major peripheral mixed function (motor and sensory) nerve ; median and ulnar nerves are usually stimulated at the wrist overlying the path of the respective nerves with 2 electrodes (needle or surface), separated by 2 cm, with the cathode proximal and the anode distal –> a square-wave electrical stimulus of 0.2 to 2ms is applied at a rate of 1 to 2Hz. –> The stimulus intensity is adjusted to produce minimal muscle contraction (usually 10 to 60mA) –> The resulting electrical potential is recorded at various points along the neural pathway from the peripheral nerve to the cerebral cortex.
👉🏿COMMON SITES OF STIMULATION:
🔻Upper extremity : median and ulnar nerves at the wrist.
🔻Lower extremity : the common peroneal nerve at the popliteal fossa and the posterior tibial nerve at the ankle.
🔻Less commonly the tongue, trigeminal nerve, and pudendal nerve have been studied.
👉🏿RECORDING:
After upper limb stimulation, potentials are recorded at the brachial plexus (Erb’s point, 2 cm superior to the clavicular head of the sternocleidomastoid muscle), the cervicomedullary junction (posterior midline of the neck at the second cervical vertebra), and the scalp overlying the somatosensory cortex on the contralateral side.
After stimulation of the lower extremity, potentials are recorded at the popliteal fossa, lumbar and cervical spinal cord, and somatosensory cortex. It is important to record nerve and subcortical potentials to verify adequate stimulation and delineate anesthetic effects.
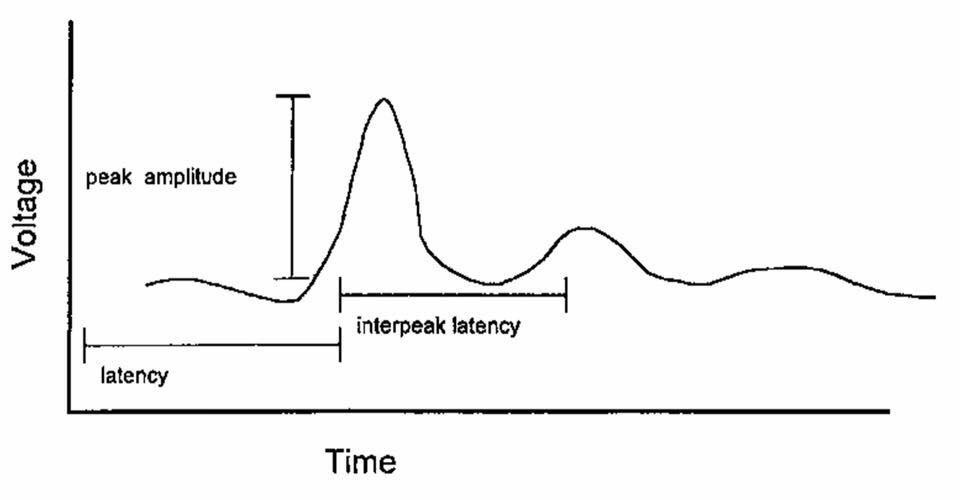
👉🏿PLOTTING:
The SSEP is plotted as a waveform of voltage vs. time.
It is characterized by:
# Amplitude (A), which is measured in microvolts from baseline to peak or peak to peak
# Latency (L), which is the time, measured in milliseconds, from onset of stimulus to occurrence of a peak or the time from one peak to another
👉🏿MORPHOLOGY:
described as positive (P, below the baseline) or negative (N, above the baseline)
A waveform is identified by the letter describing its deflection above or below the baseline followed by a number indicating its latency (e.g., N20)
👉🏿INTRAOPERATIVE SSEP’s, INDICATIVE OF SURGICAL TRESSPASS / ISCHEMIA INCLUDE
a . increased latency
b . decreased amplitude
c . complete loss
Any decrease in amplitude greater than 50% or increase in latency greater than 10% may indicate a disruption of the sensory nerve pathways. The spinal cord can tolerate ischemia for about 20 minutes before SSEPs are lost.
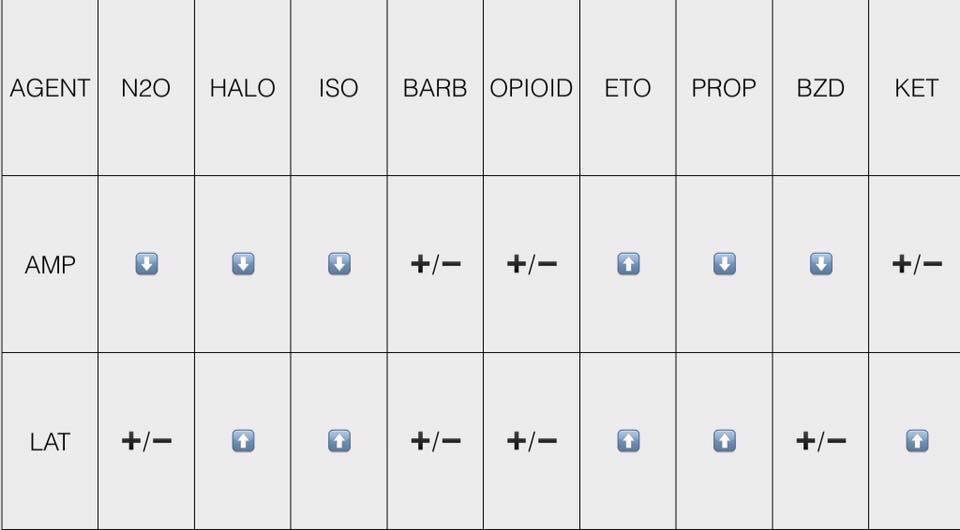
👉🏿ANESTHETIC DRUGS AND SSEP
All of the halogenated inhaled anesthetics probably cause roughly equivalent dose-dependent decreases in amplitude and increases in latency that are further worsened by the addition of 60% nitrous oxide. It is best to restrict the use of volatile anesthetics and nitrous oxide to levels below 1 minimum alveolar concentration (MAC) and not to combine the two. n If possible, bolus injections of drugs should be avoided, especially during critical stages of the surgery. Continuous infusions are preferable.
👉🏿CONDITIONS ALTERING SSEP
# Hypothermia : increases latency, whereas amplitude is either decreased or unchanged. For each decrease of 1 degree C, latency is increased by 1ms.
# Hyperthermia (4 degree C) : decreases amplitude to 15% of the normothermic value.
# Hypotension: With a decrease of the mean arterial blood pressure (MAP < 40mm Hg), progressive decreases in amplitude are seen. The same change is also seen with a rapid decline in MAP to levels within the limits of cerebral autoregulation.
# Hypoxia: ?Decreased amplitude
# Hypocarbia: Increased latency has been described at an end-tidal CO 2 < 25mm Hg.
# Isovolumic hemodilution: Latency is not increased until the hematocrit is < 15%, and amplitude is not decreased until the hematocrit is < 7%. This effect is likely caused by tissue hypoxia.
👉🏿INTRAOPERATIVE USES
🔻scoliosis surgery & Harrington rod placement
🔻spinal cord decompression and stabilisation after acute SCI spinal fusion
🔻brachial plexus exploration following acute injury
🔻resection of spinal cord tumours, cysts & vascular anomalies
🔻correction of cervical spondylosis
🔻resection of 4 th ventricular cysts
🔻release of tethered spinal cord
🔻resection of acoustic neuroma
🔻resection of intracranial lesions involving the sensory cortex
🔻resection of thalamic tumours
🔻abdominal and thoracic aneurysm repair
👉🏿IF SSEP CHANGES SIGNIFICANTLY, WHAT THE SURGEON AND ANAESTHESIOLOGIST CAN DO TO DECREASE THE INSULT?
The anesthesiologist can:
🔻Increase mean arterial blood pressure, especially if induced hypotension is used.
🔻Correct anemia, if present.
🔻Correct hypovolemia, if present.
🔻Improve oxygen tension.
🔻Correct hypothermia, if present.
The surgeon can:
🔻Reduce excessive retractor pressure.
🔻Reduce surgical dissection in the affected area.
🔻Decrease Harrington rod distraction, if indicated.
🔻Check positioning of associated instrumentation (e.g., screws, hooks).
🌀If changes in the SSEPs persist despite corrective measures, a wake-up test may be performed to confirm or refute the SSEP findings. The patient’s anesthetic level is lightened, and a clinical assessment of neurologic function is performed. The monitoring of motor-evoked potentials along with SSEPs provides a more complete assessment of neural pathway integrity. As the sensory pathways are supplied predominantly from the posterior spinal artery & the motor tracts from the anterior, a significant motor deficit can develop without significant change in SSEP’s.
#ssep ,#neuroanaesthesia , #anaesthesia , #neuromonitoring , #evokedpotential
🕶Cerebral ischemia slows neurotransmission and neuronal energy metabolism, resulting in decreased amplitude and increased latency of specific peaks.
🕶For SSEPs, a 50% reduction in amplitude and/or a 10% increase in latency [changes in the central conduction times, namely, the interpeak latencies between the N14 and N20 peaks] of SSEP signals from the baseline are generally accepted to be a significant change
🕶A 50% reduction on SEP amplitude has been shown to occur when cerebral blood flow decreases below 14 mL/100 g/min
🕶MEP have less well-defined warning criteria as compared to SSEPs; however, increased stimulus thresholds and/or decreased MEP amplitudes in relation to dramatic events (i.e., clip application) are indicative of pending neurologic insult.
🕶For BAEP, an increase in latency of more than 1 msec, particularly in wave V, is considered to be clinically significant.
🕶Unlike #EEG monitoring the evoked potential tests can detect subcortical functional status by way of perforating branches such as the anterior choroidal and medial striate arteries
Reference: Anesthesiology Research and Practice Volume 2014, Article ID 595837, Controversies in the Anesthetic Management of Intraoperative Rupture of Intracranial Aneurysm, Tumul Chowdhury, Andrea Petropolis,Marshall Wilkinson, Bernhard Schaller Nora Sandu and Ronald B. Cappellani
#neuroanaesthesia , #neuroanesthesia , #EvokedPotential , #neurosurgery , #anesthesiologist , #anesthesia .
