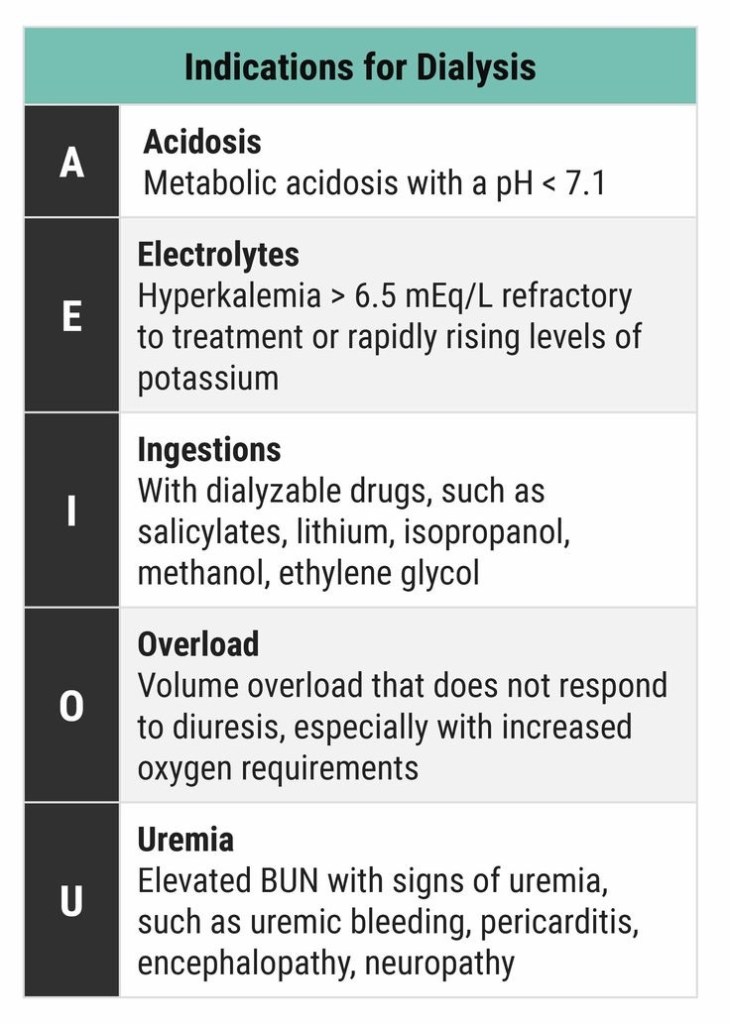
DIALYSIS INDICATIONS
NICE 2015 GUIDELINES
EUROPEAN CONSENSUS 2011 FOR INTRAOPERATIVE FLUID THERAPY
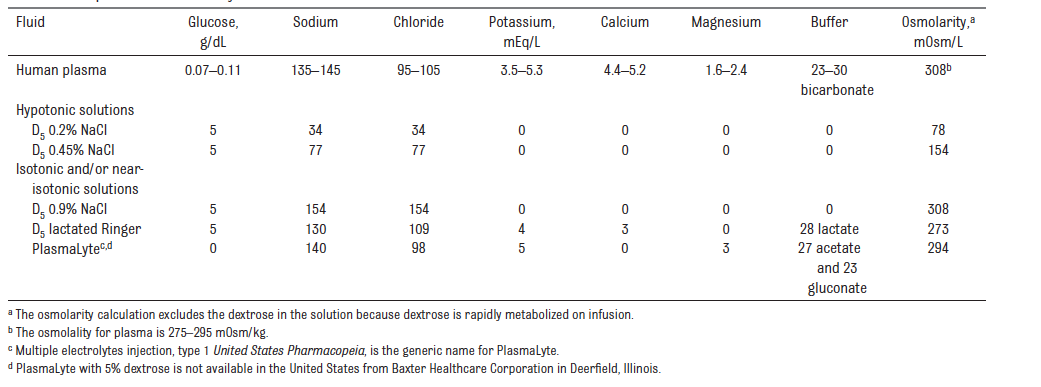
An appropriate solution for intraoperative infusion in children should have an osmolarity and sodium content close to the physiologic range in order to avoid hyponatraemia, an addition of 1–2.5% glucose in order to avoid hypoglycaemia, lipolysis or hyperglycaemia and should also include metabolic anions (i.e. acetate, lactate or malate) as bicarbonate precursors to avoid acid–base balance disturbances (i.e. hyperchloraemic acidosis). The intraoperative infusion of isotonic solutions containing 1–2.5% glucose in children is considered well established use in Europe
BELGIAN PERIOPERATIVE FLUID RECOMMENDATIONS 2012
For children undergoing uncomplicated day-case surgery or minor surgery and those expected to remain nil-by-mouth for at least 24 hours after surgery or undergoing major surgery, a full volume maintenance fluid should be administered during the intraoperative period and immediate post-operative period, as this is associated both with a reduced incidence of postoperative nausea and vomiting particularly in those children receiving opioids, and with a significantly reduced postoperative increase in ADH concentration. The latter presumed to be a result of correction of hypovolemia.
During the first postoperative day, decreased volumes of the maintenance fluid consisting of an isotonic solution at two-thirds or 70% of the calculated maintenance rate is recommended, provided the child is normovolemic.
This solution would preferably be enriched with glucose 5% (50 ml glucose 50% in 500 ml fluid) in order to provide an adequate caloric supply as recommended (4 to 8 mg glucose/kg/min). In addition, the osmolarity of such a solution makes it possible to be administered on a peripheral venous access.
Recognizing that fluids used to replace ongoing losses should reflect the electrolyte composition of fluid lost, NaCl 0.9% has been considered as appropriate in most cases. Isotonic fluids including colloids are to be used as a bolus in the event of hypovolemia.
Consider iv. fluids as medications.
Administer isotonic fluids (saline 0.9%, Plasmalyte®, Hartmann® or colloids) as a bolus in the event of hypovolemia.
Monitoring plasma electrolytes and glucose concentrations regularly i.e. once daily or more if clinically indicated (documented plasma [Na] < 135 mmol/L)
AMERICAN ACADEMY OF PAEDIATRICS 2018
The American Academy of Pediatrics recommends that patients 28 days to 18 years of age requiring maintenance IVFs should receive isotonic solutions with appropriate potassium chloride and dextrose because they significantly decrease the risk of developing hyponatremia. (For the purposes of this guideline, isotonic solutions have a sodium concentration similar to PlasmaLyte, or 0.9% NaCl)
APA CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN 2007/ 2010 REVIEW
EXECUTIVE SUMMARY
1. Children can safely be allowed clear fluids 2 hours before surgery without increasing the risk of aspiration.
2. Food should normally be withheld for 6 hours prior to surgery in children aged 6 months or older.
3. In children under 6 months of age it is probably safe to allow a breast milk feed up to 4 hours before surgery
4. Dehydration without signs of hypovolaemia should be corrected slowly.
5. Hypovolaemia should be corrected rapidly to maintain cardiac output and organ perfusion.
6. In the child, a fall in blood pressure is a late sign of hypovolaemia.
7. Maintenance fluid requirements should be calculated using the formula of Holliday and Segar
8. A fluid management plan for any child should address 3 key issues
i. any fluid deficit which is present
ii. maintenance fluid requirements
iii. any losses due to surgery e.g. blood loss, 3rd space losses
9. During surgery all of these requirements should be managed by giving isotonic fluid in all children over 1 month of age
10. The majority of children over 1 month of age will maintain a normal blood sugar if given non-dextrose containing fluid during surgery
11. Children at risk of hypoglycaemia if non-dextrose containing fluid is given are those on parenteral nutrition or a dextrose containing solution prior to theatre, children of low body weight (<3rd centile) or having surgery of more than 3 hours duration and children having extensive regional anaesthesia. These children at risk should be given dextrose containing solutions or have their blood glucose monitored during surgery.
12. Blood loss during surgery should be replaced initially with crystalloid or colloid, and then with blood once the haematocrit has fallen to 25%. Children with cyanotic congenital heart disease and neonates may need a higher haematocrit to maintain oxygenation.
13. Fluid therapy should be monitored by daily electrolyte estimation, use of a fluid input/output chart and daily weighing if feasible.
14. Acute dilutional hyponatraemia is a medical emergency and should be managed in PICU.
