1.TAKE CARE OF YOURSELF 2.ASK OPINION TO SOMEONE WHO ALREADY HAD AN EXPERIENCE 3.GOOD COMMUNICATION BETWEEN ANESTHESIA & SURGERY TEAMS 4.PLAN SUFFICIENTLY EARLY AND DISCUSS INSIDE THE TEAM 5.ASSIGN DUTIES CLEARLY TO EACH MEMBER
GENERAL INSTRUCTIONS FOR PERIOPERATIVE SCENARIO (Source: 1 Consensus guidelines for managing the airway in patients with COVID-19 Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists, Source: 2 Editorial, anesthesia-analgesia, May 2020, Source: 3 Anesthesia Patient Safety Foundation and World Federation of Societies of Anesthesiologists, accessed 3/13/2020, Source: 4 Interim guidance for health care providers during covid-19 outbreak from AHA and 5 CDC guidelines)
Remember that your personal protection is the priority. Plan ahead as it takes time to apply all the barrier precautions. Before intubation, review and practice donning and doffing the appropriate respiratory protection, gloves, face shield, and clothing.
Practice appropriate hand hygiene before and after all procedures.
Anaesthesia/ Intubating personnel should don full PPE (Well fitting N95 mask, goggles+ face shield, splash resistant gown, boot covers, double gloves)
Patient should wear a mask; continue it during pre-oxygenation
When intubated patient being transferred to ICU or transfer from one circuit / ventilator to other, avoid disconnections in patient’s breathing circuit. Put the ventilator on stand by to turn off flows. Clamp ETT with forceps to prevent aerosolization
Tracheal intubation of the COVID positive patient is a high risk procedure for the staff, irrespective of the clinical severity of the disease. Do not rush; priority should be to succeed in the first chance. Avoid unreliable, unfamiliar or repeated techniques
Know and communicate the plan before entering the room (Use a checklist). Also plan how to communicate once inside the Operating Room (OR) (It will be difficult with the PPE; You may have to use adequate volume while speaking). You can display your plan/algorithm in the OR.
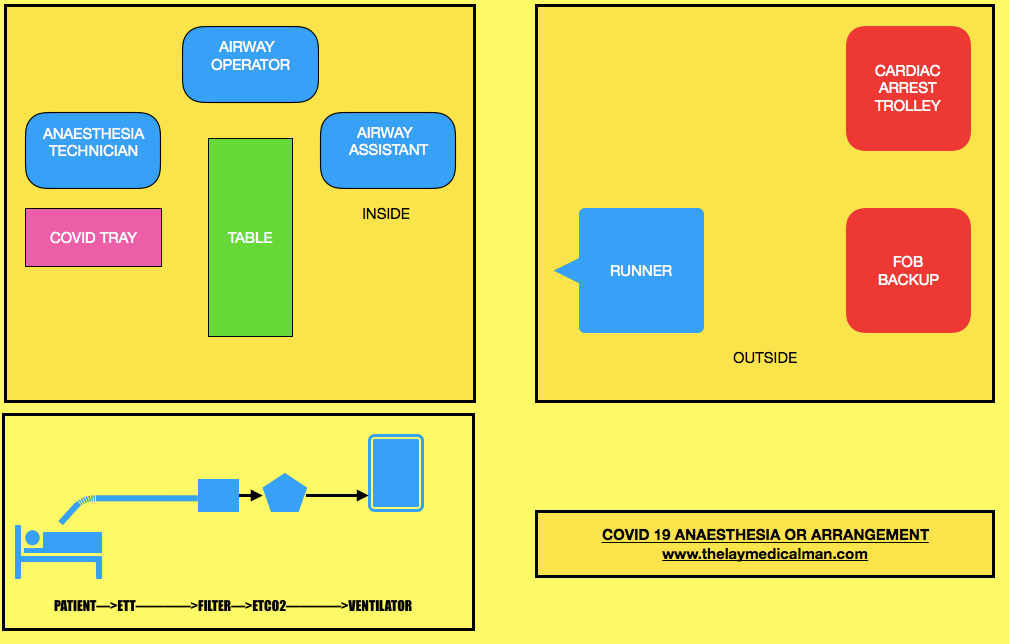
Limit staff present at the tracheal intubation: one intubator, one assistant and one to give drugs, equipments and monitor the patient; A runner should be there outside the room. The most experienced anaesthetist available should perform the intubation, to maximise first-pass success. Technician/assistant to keep a distance of 2 m from patient
Touch as less as possible once inside the room
Ideally we should intubate in a negative pressure room with >12 air changes per hour
If this is not available, switch off air conditioner/ positive pressure, 20 minutes before and 20 mins after Aerosol Generating Procedures
PREPARATION OF DRUG/ EQUIPMENT
PROCEDURE:
Most of this should happen outside the room
Pre-procedure machine check to ensure no leak. Check circuit
Create a COVID Intubation Trolley (This can also be used in the ICUs)
Arrange N95 mask and 2 HEPA filters to attach between tracheal tube and breathing circuit and between expiratory limb and anaesthesia machine
Standard monitors, cannulas, instruments, drugs
If patient is on HCQ, it will be better to avoid glycopyrrolate and ondansetron
Sterile plastic covers: for protecting monitors, ventilator or anaesthesia machine and for covering the cable covering the laryngoscope handle. Also keep stylet, appropriate size cuffed tube,10 ml syringe for cuff inflation, oral suction catheter etc
Face mask
Airways
A second generation Supra Glottic Airway device for airway rescue
Use 5 minutes of preoxygenation with 100% oxygen and RSI techniques to avoid manual ventilation of patient’s lungs and the potential aerosolization of virus from airways.
No bag mask manual ventilation. Holding the mask: 2-person, 2-handed, with a VE grip technique (rather than the C- technique) to improve seal. If you are forced to mask ventilate, use a 2-person, low flow, low pressure technique
Intubating dose of Rocuronium or Suxamethonium should be given along with propofol or ketamine (can avoid cardiovascular collapse in some situations): Intubate after 90 seconds (prevent coughing)
Indirect laryngoscopy with video laryngoscope & intubation under the transparent plastic sheet on the patient
Inflate the ETT cuff immediately after tube placement, before starting ventilation
HEPA shield antiviral filter connected to ETT & then connect ETT to ventilator breathing circuit
Avoid all Aerosol Generating Procedures (AGP) like high flow nasal oxygen, NIV, bronchoscopy and tracheal suction without a closed suction facility. Routine use of supraglottic airway devices unless in unanticipated difficult airway should be avoided
Use a closed suction system
Confirm correct position of the tracheal tube. Confirmation of the ETT position will be difficult while wearing PPE; so for this purpose we may have to rely on inspection of bilateral chest examination, observation of ETCO2 waveforms etc.
Have a vasopressor ready for managing hypotension if it happen post-intubation
Push-twist all connections to avoid circuit disconnections
Clamp tube and pause ventilator for all airway manoeuvres and for attempting to resolve circuit disconnections
Place a nasogastric tube if necessary.
If COVID-19 status has not been confirmed, take a deep tracheal aspirate using closed suction
Institute mechanical ventilation and stabilize patient, as appropriate.
Lung protective ventilation strategies: Small TV:6 ml/Kg [Predicted body wt= Ht in cm-100 (males) & Ht- 110 (females)]. Plateau pressure </= 30 cm H2O. PEEP= 10-15 mm Hg, Adjust FiO2 to achieve reasonable PaO2 (>60 mm Hg). Target SaO2 88-95%. pH >/= 7.25 (Permissive Hypercapnia)
Use only metered dose inhalers if bronchodilators indicated at any point ( avoid nebulisation)
Use of intravenous anesthesia would be preferred to the use of a volatile gas anesthetic machine in the ICU environment, especially given that many of these patients are not going to be rapidly recovered and extubated following the procedure. (Source:6)
Rule out pneumothorax if there is difficulty in ventilation ( Lung USG, CXR)
Clean the room 20 minutes after tracheal intubation or any AGP.
All efforts to prevent coughing including lidocaine/dexmedetomidine
To prevent aerosol generation extubation also should be performed under transparent sheet
O2 by nasal cannula / face mask. When wearing nasal prongs, a surgical mask can be worn by the patient over the prongs to reduce droplet spread. Should higher oxygen requirements necessitate use of a mask, non-rebreather masks with an attached exhalation filter can be used.
NIV or High flow O2 can cause aerosol generation: so better to avoid
Ensure the availability of ambu bag with filter during transfer
After leaving the room, do a meticulous doffing of PPE
In the ICU: The use of CPAP/BiPAP may increase the risk of delayed deterioration leading to need for emergent intubation and increased risk of mistakes in donning PPE due to time pressures to resuscitate. In general, CPAP/BiPAP should be avoided in patients with Covid 19 and should never be used outside of appropriate airborne/droplet isolation.
All airway equipment must be decontaminated and disinfected according to appropriate hospital policies.
After removing protective equipment, avoid touching hair or face before washing hands.
NB: N95 mask disinfection: Either cycle through 4 masks in series: one for each day, then repeat (OR heat the mask to 70 degree for 30 minutes (UV light, alcohol, bleach and touching the metal of the oven during heating…all these can degrade the mask)
EMERGENCY INTUBATION IN THE CRITICAL CARE UNIT (Source: 6 Wax, R.S., Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth/J Can Anesth(2020))
Here also the same principles cited above should apply; additional points are
Higher level of precautions are needed here as there is high-level viral shedding due to severity of patient illness and procedures associated with resuscitation or intubation may generate aerosols
All personnel in the room must be using appropriate PPE, including either a fit-tested N95 mask or a PAPR. The procedure should be attempted by the most skilled person. Recurrent traffic of people bringing equipment into the room may increase the risk of viral transmission.
Clinicians should strongly consider pneumothorax in any ventilated patient with sudden respiratory deterioration. Portable ultrasound may be used to quickly assist in the diagnosis of a pneumothorax, as arranging for a CXR will lead to delay in intervention.
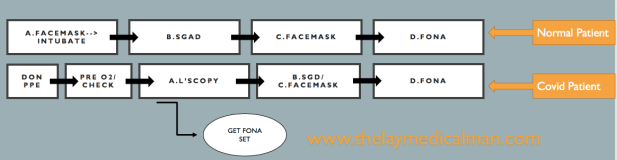
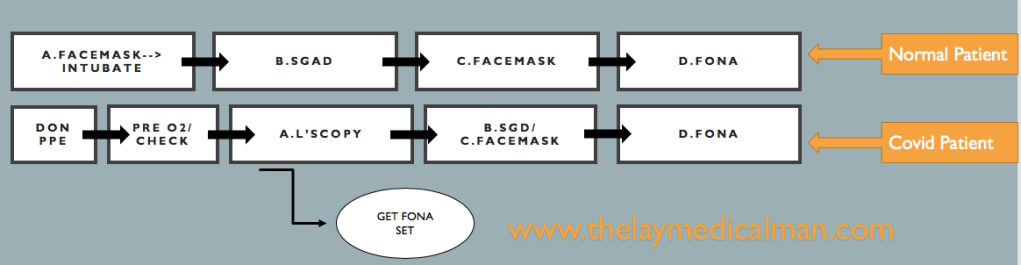
DIFFICULT AIRWAY
Compared to the normal patient, after the first failure of intubation itself, we should order for Front Of Neck Access (FONA) set. And in the next step, we can either do step B (SGD) or step C ( Facemask). Because of this, we will move fast towards the final step of FONA in the Covid difficult airway algorithm.
DIFFICULT AIRWAY: NORMAL PATIENT VS COVID PATIENT
Prevention and management of respiratory or cardiac arrest: Protected Code Blue (PCB)(Source: 7 Resuscitation Council. Resuscitation Council UK Statement on COVID-19 in relation to CPR and resuscitation in healthcare settings. 2020. Source: 8 Wax, R.S., Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth/J Can Anesth(2020))
Do not listen or feel for breathing by placing your ear and cheek close to the patient’s mouth
Full Aerosal Generating Procedure (AGP) Personal Protective Equipment (PPE) must be worn by all members of the resuscitation/emergency team before entering the room.
Sets of AGP PPE must be readily available where resuscitation equipment is being locally stored.
No chest compressions or airway procedures such as those detailed below should be undertaken without full AGP PPE.
Once suitably clothed, start compression-only CPR and monitor the patient’s cardiac arrest rhythm as soon as possible.
Do not do mouth-to-mouth ventilation or use a pocket mask. If the patient is already receiving supplemental oxygen therapy using a face mask, leave the mask on the patient’s face during chest compressions as this may limit aerosol spread.
If not in situ, but one is readily available, put a simple oxygen mask on the patient’s face. Restrict the number of staff in the room (if a single room). Allocate a gatekeeper to do this.
Tracheal intubation or SGA insertion must only be attempted by individuals who are experienced and competent in this procedure.
Dispose of, or clean, all equipment used during CPR following the manufacturer’s recommendations and local guidelines.
Any work surfaces used for airway/resuscitation equipment will also need to be cleaned according to local guidelines.
Specifically, ensure equipment used in airway interventions (e.g. laryngoscopes, face masks) is not left lying on the patient’s pillow, but is instead placed in a tray.
Do not leave the Yankauer sucker placed under the patient’s pillow; instead, put the contaminated end of the Yankauer inside a disposable glove.
Lower risk resuscitation interventions:
Placement of an oral airway
Placement of an oxygen mask with exhalation filter on patient (if available)