Category Archives: Neuroanesthesia
Awake Craniotomy: Decoding a misnomer!
TIVA IN NEUROANAESTHESIA
Anesthesia / Medical implications of Von Hippel–Lindau disease (vHLD)
vHLD usually presents in young adults with cerebellar, medullary or spinal haemangioblastomas, retinal angiomatosis, renal cell carcinoma and phaeochromocytoma
The frequency of phaeochromocytomas is 7–20%
About 25% of patients with CNS haemangioblastomas subsequently turn out to have vHLD.
Erythrocytosis and a high haematocrit are common and has to be searched for.
Surgery for one manifestation of the disease may be complicated by the presence of an undiagnosed #phaeochromocytoma. In this situation, pharmacological control of phaeochromocytoma should get more priority and surgery may have to be carried out in two stages
Spinal Anaesthesia may be dangerous in the presence of an undiagnosed cerebral or spinal tumour. Another point is, spinal cord haemangioblastomas can occur at more than one level. An MRI if already done, can help us to take a proper decision.
Pregnancy may worsen the disease, by increasing the vascularity of tumours. Urgent and life saving neurosurgical intervention may become necessary: for e.g. when a spinal tumor bleeds, when a tumor obstructs CSF flow and causes acute hydrocephalus. Sometimes elective procedures like removal of a phaeochromocytoma which became evident during pregnancy has to be removed. It may become necessary to carry out these procedures during pregnancy or along with a Caesarean section.
Surgery may be required for more than one lesion at the same time.
So careful assessment should be made for lesions other than the one for which anaesthesia is required, and in particular for any symptoms and signs of cerebral, cerebellar or spinal cord tumours and phaeochromocytoma.
In the situation in which two lesions are present, decisions may have to be made as to whether to operate simultaneously or separately . During pregnancy the management of the delivery must be carefully planned in advance.
Although 24-h urinary screening for catecholamines can be performed, plasma normetanephrines and metanephrines are the most sensitive tests for detecting phaeochromocytomas in patients with family predisposition
Reference: Anaesthetic management of a patient with von Hippel–Lindau disease: a combination of bilateral phaeochromocytoma and spinal cord haemangioblastoma. European Journal of Anaesthesiology 13: 81–3. , Anesthesia Databook, 3rd edition
THE SPECIFIC MECHANISMS OF ACTION OF #MANNITOL IN VARIOUS CLINICAL SITUATIONS
Mannitol is a monosaccharide available as 10% & 20% solutions
DURING NEUROSURGERY/ IN NEUROCRITICAL CARE:
✔️Mannitol is freely filtered in the glomerulus but won’t get reabsorbed in the tubules; so it will drive water from the interstitium which gets eliminated as urine. Hence acts as an osmotic diuretic
✔️When blood brain barrier is intact, the osmotic gradient created by mannitol will move water from the cerebral extravascular compartment to the intravascular space, reducing ICP. If blood brain barrier is not intact, it will worsen cerebral edema.
✔️The expansion of the plasma volume caused by mannitol will reduce the viscosity and improve cerebrovascular microcirculation and oxygenation. The increase in cardiac output can also cause an increase in regional blood flow which will cause a compensatory cerebrovascular vasoconstriction in areas where autoregulation is intact.
IN CRUSH INJURY / MYOGLOBINURIA
✔️Will release renal prostaglandins, which will cause renal vasodilation and increase tubular urine flow causing a solute washout and avoidance of tubular obstruction #TheLayMedicalMan
MECHANISM BEHIND ADVERSE EFFECTS
✔️The initial increase in plasma volume as a result of drawing of water into the vascular component and the resultant increase in cardiac output can precipitate heart failure in cardiac patients
✔️The osmotic diuresis can cause hypernatremia [increases urinary losses of both sodium and electrolyte-free water] , metabolic acidosis and hyperosmolarity. It has been advised that therapy should be monitored and titrated so that osmolarity doesn’t go up beyond 300 mOsm/L
✔️The rise in the plasma potassium concentration following hypertonic mannitol is due to the movement of potassium out of the cells into the extracellular fluid as the rise in cell potassium concentration induced by water loss favors passive potassium exit through potassium channels in the cell membrane
✔️Though it has been used for renal protection, the reduction in renal perfusion resulting from hypovolemia caused by diuresis can adversely affect renal function; so should be avoided in patients with renal dysfunction
#Neuroanesthesia , #Anesthesia , #Neurology , #CriticalCare
BRIEF FUNCTIONAL ANATOMY OF THE BRAIN
✔️Precentral gyrus contains the primary motor cortex
✔️Premotor cortex lies immediately anterior to Primary motor cortex ( Brodmann’s area 6 on the lateral surface of the frontal lobe.)
✔️Premotor cortex is active in response to EXTERNAL visual or somatic sensory cues (e.g. reaching for an object in full view, or identifying an object by touch alone). Also has role in bilateral postural fixation (e.g. stabilization of the hips during walking).
✔️The supplementary motor area occupies a neighbouring part of Brodmann’s area 6 on the medial surface of the frontal lobe.
✔️The supplementary motor area seems to respond to INTERNAL cues, especially intentions to make voluntary movements (even if the movement is not carried out).
✔️Lesions of the supplementary motor cortex are associated with contralateral inability to initiate movements (akinesia).
✔️The inferior frontal gyrus of the dominant hemisphere (usually the left) contains the (Broca’s) motor speech area (Brodmann’s areas 44 and 45)
✔️The somatic sensory cortex, occupies the entire postcentral gyrus (Brodmann’s areas 3, 1 and 2, rostral to caudal).
✔️ Caudal to the somatosensory cortex is the sensory association cortex, which is divided into a superior and an inferior parietal lobule by an intraparietal sulcus.
✔️ The superior lobule is thought to be responsible for conscious awareness of the contralateral half of the body. Lesions of this part of the cortex may result in neglect of the contralateral side of the body.
✔️ The inferior lobule in the dominant (usually left) hemisphere is associated with language functions.
✔️ The cortex adjacent to the parieto-occipital sulcus and the calcarine sulcus, which lies on the medial surface of occipital lobe, constitutes the primary visual cortex (Brodmann’s area 17).
✔️ The superior surface of the temporal lobe contains the primary auditory cortex (Brodmann’s areas 41 and 42), responsible for the conscious perception of sound. Unilateral lesions of the primary auditory cortex will therefore cause partial deafness in both ears.
✔️ The auditory association cortex, known as Wernicke’s area corresponds to Brodmann’s area 22 in the dominant hemisphere. It allows for understanding of the spoken word, and connects with other language areas of the brain.
✔️ The temporal lobe curls inward to form the hippocampus which lies in the floor of the inferior horn of the lateral ventricle, and forms part of the limbic system. Its functions relate to short-term memory and the emotional aspects of behaviour.
✔️ Lying close to the anterior end of the hippocampus is the amygdala. Its a mass of subcortical grey matter that also forms part of the limbic system. It is associated with the conscious appreciation of smells.
✔️ The insula is one of the cortical centres for pain, and is also involved in involuntary activities such as the control of viscera by the autonomic nervous system.
✔️ The basal ganglia includes
• striatum (caudate nucleus, putamen of the lentiform nucleus and the nucleus accumbens)
• pallidum (globus pallidus of the lentiform nucleus)
• subthalamic nucleus
• compact part of the substantia nigra
✔️ Four basic circuits are known to occur from the cerebral cortex, through the basal ganglia and back to the cortex, by a direct or indirect route:
-a motor loop is concerned with learned movements;
-a cognitive loop with motor intentions;
-a limbic loop with emotional aspects of movement and
-an oculomotor loop with voluntary saccades.
✔️ Limbic system is composed of the the parahippocampal and cingulate gyri, the septal area, the hippocampal formation and the amygdala. Declarative memory (i.e. of new facts and events) may occur as modifications of synapses within the hippocampus.
✔️ Diencephalon comprises, from superior to inferior, the epithalamus, thalamus, subthalamus and hypothalamus.
✔️ The thalamus is the largest component of the diencephalon and is composed of numerous nuclei.
✔️ The epithalamus consists principally of the pineal gland that secretes melatonin and is involved with circadian rhythm and regulation of the onset of puberty and the habenular nuclei.
✔️ The subthalamus contains the subthalamic nucleus which connects to the globus pallidus and substantia nigra and is involved with the control of movement.
✔️ The hypothalamus has important connections with the limbic system, a controlling influence on autonomic nervous system activity and a role in neuroendocrine function.
✔️ The cerebellum coordinates movement by maintenance of equilibrium, posture and muscle tone at an unconscious level. Also concerned with muscular coordination, including trajectory, speed and force of movements.
✔️ The tectum (roof) of the midbrain is formed by four colliculi –the paired superior colliculi are associated with the visual system, and the inferior colliculi with the auditory system.
#FunctionalAnatomy, #NeuroAnatomy, #NeuroAnesthesia, #Neurosurgery ,#brain
Reference: The brain: functional divisions, Leo Donnelly, Neurosurgery, Neuroradiology & Neurocritical Care in Anaesthesia
BE SENSITIVE ENOUGH TO SENSE SSEP (SOMATO SENSORY EVOKED POTENTIAL)❗️❗️
SSEP reflect the ability of a specific neural pathway to conduct an electrical signal from the periphery to the cerebral cortex.
👉🏿THIS IS WHAT WE DO:
A skin surface electrode is placed near a major peripheral mixed function (motor and sensory) nerve ; median and ulnar nerves are usually stimulated at the wrist overlying the path of the respective nerves with 2 electrodes (needle or surface), separated by 2 cm, with the cathode proximal and the anode distal –> a square-wave electrical stimulus of 0.2 to 2ms is applied at a rate of 1 to 2Hz. –> The stimulus intensity is adjusted to produce minimal muscle contraction (usually 10 to 60mA) –> The resulting electrical potential is recorded at various points along the neural pathway from the peripheral nerve to the cerebral cortex.
👉🏿COMMON SITES OF STIMULATION:
🔻Upper extremity : median and ulnar nerves at the wrist.
🔻Lower extremity : the common peroneal nerve at the popliteal fossa and the posterior tibial nerve at the ankle.
🔻Less commonly the tongue, trigeminal nerve, and pudendal nerve have been studied.
👉🏿RECORDING:
After upper limb stimulation, potentials are recorded at the brachial plexus (Erb’s point, 2 cm superior to the clavicular head of the sternocleidomastoid muscle), the cervicomedullary junction (posterior midline of the neck at the second cervical vertebra), and the scalp overlying the somatosensory cortex on the contralateral side.
After stimulation of the lower extremity, potentials are recorded at the popliteal fossa, lumbar and cervical spinal cord, and somatosensory cortex. It is important to record nerve and subcortical potentials to verify adequate stimulation and delineate anesthetic effects.
👉🏿PLOTTING:
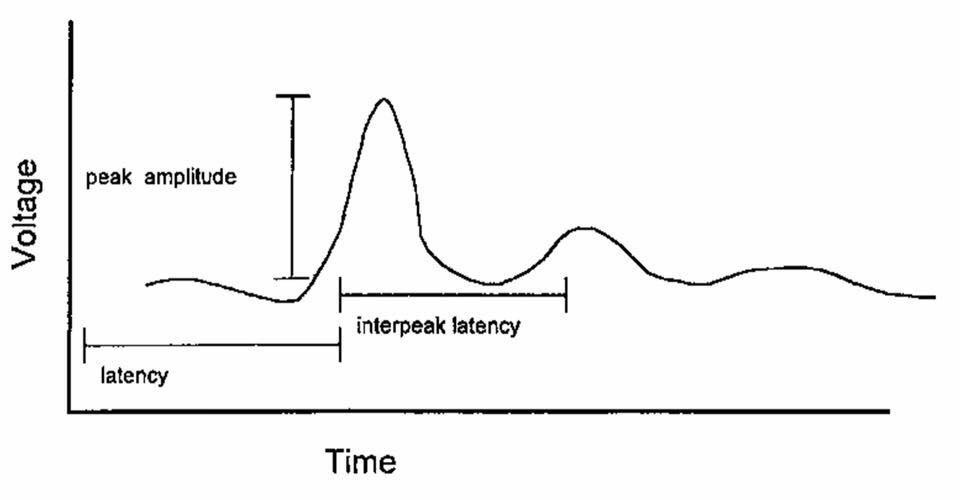
The SSEP is plotted as a waveform of voltage vs. time.
It is characterized by:
# Amplitude (A), which is measured in microvolts from baseline to peak or peak to peak
# Latency (L), which is the time, measured in milliseconds, from onset of stimulus to occurrence of a peak or the time from one peak to another
👉🏿MORPHOLOGY:
described as positive (P, below the baseline) or negative (N, above the baseline)
A waveform is identified by the letter describing its deflection above or below the baseline followed by a number indicating its latency (e.g., N20)
👉🏿INTRAOPERATIVE SSEP’s, INDICATIVE OF SURGICAL TRESSPASS / ISCHEMIA INCLUDE
a . increased latency
b . decreased amplitude
c . complete loss
Any decrease in amplitude greater than 50% or increase in latency greater than 10% may indicate a disruption of the sensory nerve pathways. The spinal cord can tolerate ischemia for about 20 minutes before SSEPs are lost.
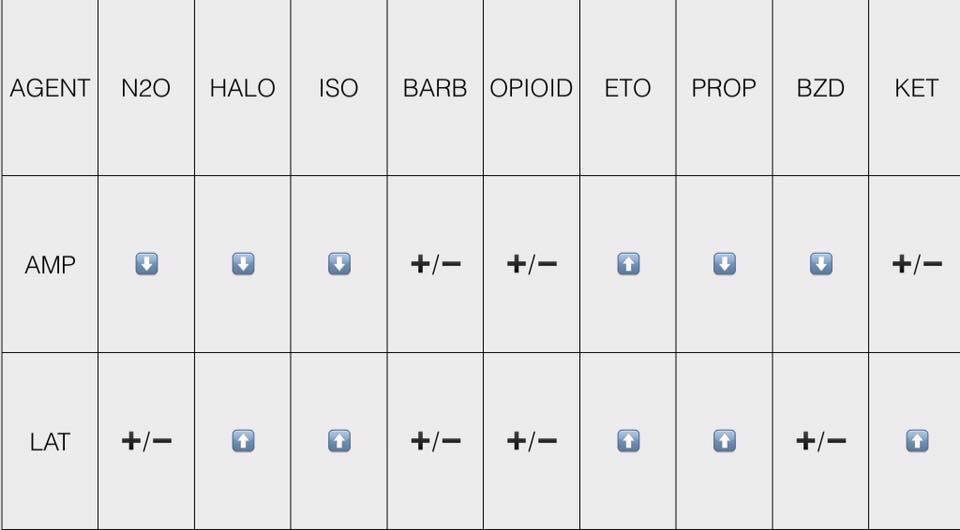
👉🏿ANESTHETIC DRUGS AND SSEP
All of the halogenated inhaled anesthetics probably cause roughly equivalent dose-dependent decreases in amplitude and increases in latency that are further worsened by the addition of 60% nitrous oxide. It is best to restrict the use of volatile anesthetics and nitrous oxide to levels below 1 minimum alveolar concentration (MAC) and not to combine the two. n If possible, bolus injections of drugs should be avoided, especially during critical stages of the surgery. Continuous infusions are preferable.
👉🏿CONDITIONS ALTERING SSEP
# Hypothermia : increases latency, whereas amplitude is either decreased or unchanged. For each decrease of 1 degree C, latency is increased by 1ms.
# Hyperthermia (4 degree C) : decreases amplitude to 15% of the normothermic value.
# Hypotension: With a decrease of the mean arterial blood pressure (MAP < 40mm Hg), progressive decreases in amplitude are seen. The same change is also seen with a rapid decline in MAP to levels within the limits of cerebral autoregulation.
# Hypoxia: ?Decreased amplitude
# Hypocarbia: Increased latency has been described at an end-tidal CO 2 < 25mm Hg.
# Isovolumic hemodilution: Latency is not increased until the hematocrit is < 15%, and amplitude is not decreased until the hematocrit is < 7%. This effect is likely caused by tissue hypoxia.
👉🏿INTRAOPERATIVE USES
🔻scoliosis surgery & Harrington rod placement
🔻spinal cord decompression and stabilisation after acute SCI spinal fusion
🔻brachial plexus exploration following acute injury
🔻resection of spinal cord tumours, cysts & vascular anomalies
🔻correction of cervical spondylosis
🔻resection of 4 th ventricular cysts
🔻release of tethered spinal cord
🔻resection of acoustic neuroma
🔻resection of intracranial lesions involving the sensory cortex
🔻resection of thalamic tumours
🔻abdominal and thoracic aneurysm repair
👉🏿IF SSEP CHANGES SIGNIFICANTLY, WHAT THE SURGEON AND ANAESTHESIOLOGIST CAN DO TO DECREASE THE INSULT?
The anesthesiologist can:
🔻Increase mean arterial blood pressure, especially if induced hypotension is used.
🔻Correct anemia, if present.
🔻Correct hypovolemia, if present.
🔻Improve oxygen tension.
🔻Correct hypothermia, if present.
The surgeon can:
🔻Reduce excessive retractor pressure.
🔻Reduce surgical dissection in the affected area.
🔻Decrease Harrington rod distraction, if indicated.
🔻Check positioning of associated instrumentation (e.g., screws, hooks).
🌀If changes in the SSEPs persist despite corrective measures, a wake-up test may be performed to confirm or refute the SSEP findings. The patient’s anesthetic level is lightened, and a clinical assessment of neurologic function is performed. The monitoring of motor-evoked potentials along with SSEPs provides a more complete assessment of neural pathway integrity. As the sensory pathways are supplied predominantly from the posterior spinal artery & the motor tracts from the anterior, a significant motor deficit can develop without significant change in SSEP’s.
#ssep ,#neuroanaesthesia , #anaesthesia , #neuromonitoring , #evokedpotential
HOW EVOKED POTENTIALS BEHAVE , WHEN BRAIN SUFFERS FROM ISCHEMIA ❓
🕶Cerebral ischemia slows neurotransmission and neuronal energy metabolism, resulting in decreased amplitude and increased latency of specific peaks.
🕶For SSEPs, a 50% reduction in amplitude and/or a 10% increase in latency [changes in the central conduction times, namely, the interpeak latencies between the N14 and N20 peaks] of SSEP signals from the baseline are generally accepted to be a significant change
🕶A 50% reduction on SEP amplitude has been shown to occur when cerebral blood flow decreases below 14 mL/100 g/min
🕶MEP have less well-defined warning criteria as compared to SSEPs; however, increased stimulus thresholds and/or decreased MEP amplitudes in relation to dramatic events (i.e., clip application) are indicative of pending neurologic insult.
🕶For BAEP, an increase in latency of more than 1 msec, particularly in wave V, is considered to be clinically significant.
🕶Unlike #EEG monitoring the evoked potential tests can detect subcortical functional status by way of perforating branches such as the anterior choroidal and medial striate arteries
Reference: Anesthesiology Research and Practice Volume 2014, Article ID 595837, Controversies in the Anesthetic Management of Intraoperative Rupture of Intracranial Aneurysm, Tumul Chowdhury, Andrea Petropolis,Marshall Wilkinson, Bernhard Schaller Nora Sandu and Ronald B. Cappellani
#neuroanaesthesia , #neuroanesthesia , #EvokedPotential , #neurosurgery , #anesthesiologist , #anesthesia .
INTRACRANIAL PRESSURE ( #ICP ) MEASUREMENT & HOW IT CAN GUIDE THERAPY❓
🔸ICP data can be used to
✔️predict outcome and evolution of intracranial pathology
✔️calculate and manage cerebral perfusion pressure (CPP) [without an ICP monitor, CPP is not known].
✔️direct management strategies, and
✔️limit the use of potentially deleterious therapies.
🔸Cerebral herniation is a pressure issue and an ICP monitor may allow early detection; it is preferable to avoid herniation than to treat it
🔸Information from an ICP monitor may provide useful information to guide patient care. For example, a patient with a worrisome-appearing CT scan who does not have intracranial hypertension may not require the same degree of treatment as a patient with a similar scan but elevated ICP. Similarly, a patient with elevated ICP that is refractory to escalating management becomes an early candidate for “second tier” treatments or if very high, even withdrawal of care.
🔸ICP values have prognostic value and so it can guide management and discussions with the family about outcomes
🔸Even transient episodes of severely raised ICP and ischemia can be devastating to the traumatized brain, making it critical to accurately and continuously monitor ICP & CPP. Because insertion of intraparenchymal ICP monitors is safe, the ability to monitor CPP per se is a supportable argument for widespread ICP monitoring.
🔸Perhaps more important than a single ICP threshold may be a trend over time, ICP waveform analysis, or whether the ICP value is associated with other detrimental effects.
🔸When both ICP and brain oxygen are treated, the outcome may be better than if just ICP is treated after TBI
🔸The ICP waveform is a modified arterial pressure tracing
🔸 It has 3 peaks: P1, P2 & P3
🔸 P1 is a result of transmitted pressure from choroid plexus
🔸 The amplitude of P2 changes with brain compliance. If compliance is poor, amplitude will be high ( can even exceed that of P1) and vice versa
🔸P3 represents the dicrotic notch
🔸 Lundberg (A) or Plateau waves are steep rise of ICP to over 50 mm of Hg and lasting for 5-20 minutes; then it falls abruptly. Are Always pathological and indicates significantly reduced compliance
🔸 Lundberg (B) waves are oscillations occurring every 1-2 minutes where ICP rises to over 20-30 mm of Hg from baseline in a crescendo manner. They are supposed to be result of altered cerebral (B)lood volume and altered tone of cerebral (B)lood vessels
🔸 Lundberg (C) waves are oscillations whose amplitude is less than that of B waves and are supposed to result because of interactions between cardiac and respiratory (C)ycles. They occur also in healthy individuals
METHODS OF MEASUREMENT OF ICP
➿ Intraventricular catheter – ventriculostomy represents the “gold standard” for pressure measurement
✔️Normally placed in the frontal horn of lateral ventricle
✔️Allows therapeutic CSF drainage
✔️Creates a pathway for infection
✔️In case of the Integra Neuroscience external drainage catheter, ICP readings are based on a fluid-filled transduction system that transmits changes in ICP through a saline-filled tube to a diaphragm on a strain gauge transducer. This monitor must be leveled with the foramen of Monro (approximately the level of the external auditory canal) after insertion and should be zero-balanced daily. The level of the drain can be adjusted to allow more or less CSF drainage.
➿Subdural bolt / Catheters
✔️ less invasive
✔️ Bolts commonly use fiberoptic technology that allows continuous ICP monitoring without CSF drainage. The fiberoptic type of catheter can be placed in the subdural space or in the brain parenchyma
✔️ Usually subdural space over frontal lobe of non-dominant hemisphere is selected
✔️ Prone to signal damping and calibration drift
✔️ Potential risk of infection
✔️ Doesn’t require penetration of brain tissue
✔️Camino Post Craniotomy Subdural Pressure Monitor utilizes the craniotomy bur holes and flap as a point of entry. The monitor is zero-balanced and then tunneled under the scalp toward the craniotomy bur hole of choice and positioned in the subdural space. This monitor contains a microtransducer at the tip, which is similar to the OLM ICP monitor ( see below)
✔️Gaeltec ICT/B pressure sensor is intended to monitor ICP subdurally. It contains a balloon-covered pressure sensor that is activated when filled with air. This monitor is self–zero-balanced in vivo and is reusable.
➿Intracerebral transducer
✔️Parenchymal devices are easier to place, particularly when altered ventricular anatomy may limit ventricular catheter placement.
✔️However, intraparenchymal fiber-optic and electronic strain gauge systems are more expensive and cannot be recalibrated once in situ
✔️Inability to check zero calibration & drain CSF
✔️ Risk of infection
✔️Less reliable
✔️The Camino OLM ICP monitor measures ICP in the intraparenchymal tissue or subarachnoid space. It contains a transducer at the distal tip, thus measuring pressure without a fluid-filled system. The catheter is secured to the skull through an adjustable bolt, allowing placement at variable depths (up to 5 cm).
✔️The Codman Microsensor catheter can be used as an intraparenchymal or intraventricular monitor, depending on the depth of the catheter
✔️ Spiegelberg ICP monitors measure ICP through an air-pouch system attached to a pressure transducer connected to an electronic device. The probes differ, depending on where they rest (Epidural or Intraparenchymal)
🔸The incidence of infection ~ 2-7% with monitoring ≥ 5 days
🔸The risks are slightly greater with dural penetration
🔸The zero reference point of the transducer is usually taken as the external auditory meatus
🔸 Rather than the waveform type, the important factors appear to be the degree and duration of ICP elevation
🔸Two emerging non-invasive ICP monitoring methods include measuring the optic nerve sheath diameter (ONSD) as seen on an ultrasound probe placed on the superolateral aspect of the orbit and the pulsatility index (PI) which is cal- culated from transcranial Doppler studies (TCD).
#NeuroAnesthesia , #anaesthesia , #TheLayMedicalMan , #NeuroCriticalCare , #CriticalCare , #NeuroICU
ICTAL BRADYCARDIA AND ASYSTOLE : AN ENTITY ALL ANESTHESIOLOGISTS SHOULD KEEP IN MIND WHEN SEEING BRADYCARDIA IN A PATIENT WITH EPILEPSY
📌Ictal bradycardia/asystole is a poorly recognised cause of collapse late in the course of a typical complex partial seizure
📌It is important to identify ictal bradycardia as a potential harbinger of lethal rhythms, such as asystole, as this may be one important mechanism leading to sudden unexpected death in epilepsy (SUDEP)
📌Tachycardia is the most common rhythm abnormality occurring in 64–100% of temporal lobe seizures. Ictal bradycardia has been reported in less than 6% of patients with complex partial seizures
📌The ictal bradycardia syndrome occurs in mostly in patients with temporal lobe seizures.
📌It is believed that abnormal neuronal activity during a seizure can affect central autonomic regulatory centres in the brain leading to cardiac rhythm changes.
📌Ictal bradycardia/asystole may be unrecognised until documented during video-electroencephalograph (video EEG)–electrocardiogram (ECG) monitoring in those with refractory epilepsy, often in the context of pre-surgical evaluation
📌Other rhythm abnormalities which can occur are change in heart rate variability, ictal tachycardias and atrioventricular (AV) block
📌If sufficiently severe, the ictal-induced bradyarrhythmia temporarily impairs both cerebral perfusion and cortical function; the result has the dual effect of terminating the seizure, while at the same time triggering syncope with consequent loss of consciousness and postural tone. In essence, a complex partial seizure patient may manifest both seizure and syncope features during the same episode.
📌There are currently no guidelines on who should undergo further cardiovascular investigations ; dual chamber pacemaker implantation has been suggested as a treatment in the long term, for epilepsy patients who manifest this syndrome and suffer repeated falls; but there is not much mention in literature both about diagnosis and about pharmacological and non pharmacological interventions to counter such episodes when presenting as an emergency situation in the perioperative scenario , especially when the patient is under anesthesia.
#Neurology , #NeuroCriticalCare , #Anesthesia , #LayMedicalMan , #CriticalCare , #Epilepsy , #Cardiology , #CardiacAnesthesia
Reference: Ictal bradycardia and atrioventricular block: a cardiac manifestation of epilepsy; Salman S. Allana Hanna N. Ahmed Keval Shah Annie F. Kelly, Oxford Medical Case Reports, British Journal of Cardiology : Ictal Bradycardia and Asystole Associated with Intractable Epilepsy: A Case Series Elijah Chaila, Jaspreet Bhangu, Sandya Tirupathi, Norman Delanty; Ictal Asystole-Life-Threatening Vagal Storm or a Benign Seizure Self-Termination Mechanism? David G. Benditt, Gert van Dijk, Roland D. Thijs (Editorial:Circulation )
