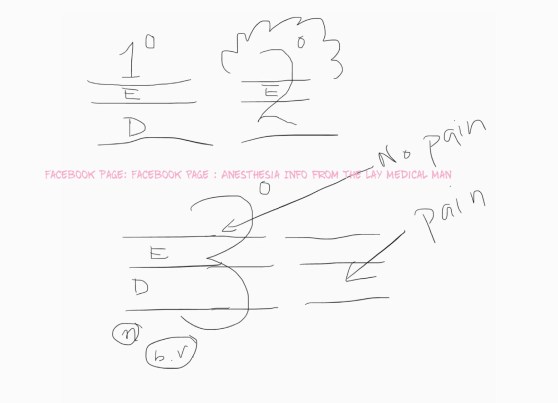
- First degree burns don’t penetrate the epidermis and the areas of involvement should not be considered when calculating for fluid volume for resuscitation
- Second degree burns penetrates the epidermis & extends into the dermis and will cause blisters
- Third degree burns involve epidermis, full thickness of dermis, deeper tissues, blood vessels and nerves
- The “rule of nines” is used to calculate the total body surface area (TBSA) .
- The Parkland formula recommends 4 mL/kg/% TBSA burned, to be given in the first 24 hours (half of this should be given in the first 8 hours and the rest over the following 16 hours).
- The Modified Brooke protocol recommends 2 mL/kg/%TBSA.
- Fluid leak may occur when patients are given volume beyond the intended calculations. This can lead to abdominal compartment syndrome, pulmonary edema, or pneumonia.
- Carbon monoxide (CO) poisoning should be considered in all major burn injuries.
- CO binds to hemoglobin (HbCO) with an affinity of 250 times that of oxygen and shifts the oxygen–hemoglobin dissociation curve to the left.
- Pulse oximetry causes falsely elevated oxygen saturation because it is unable to distinguish HbO from HbCO, as CO-Hb has similar absorption spectra as that of oxy-Hb
- HbCO levels below 10% are not usually clinically significant, levels of 20% may require mechanical ventilation, and death from CO poisoning occurs at HbCO levels of 60%.
- In cases where CO poisoning is suspected, treatment should be with highflow 100% oxygen, which increases the speed of elimination of CO. Hyperbaric chambers are used to further increase the speed of CO removal.
- Burns patients have an inability to regulate body temperature and must be kept warm.
- Urgent airway management may be indicated by the presence of a hoarse voice, dyspnea, tachypnea, or altered level of consciousness.
- Succinylcholine can cause lethal elevations in potassium after the first 48 hours.


Thanx
LikeLike