- Helpful MNEMONICS: ‘PRIP ABCDEFGHI’. Also in inspiratory films the level of the diaphragm is at the level of ribs 5/6 anteriorly and 8/10 posteriorly. (AR6PR10).
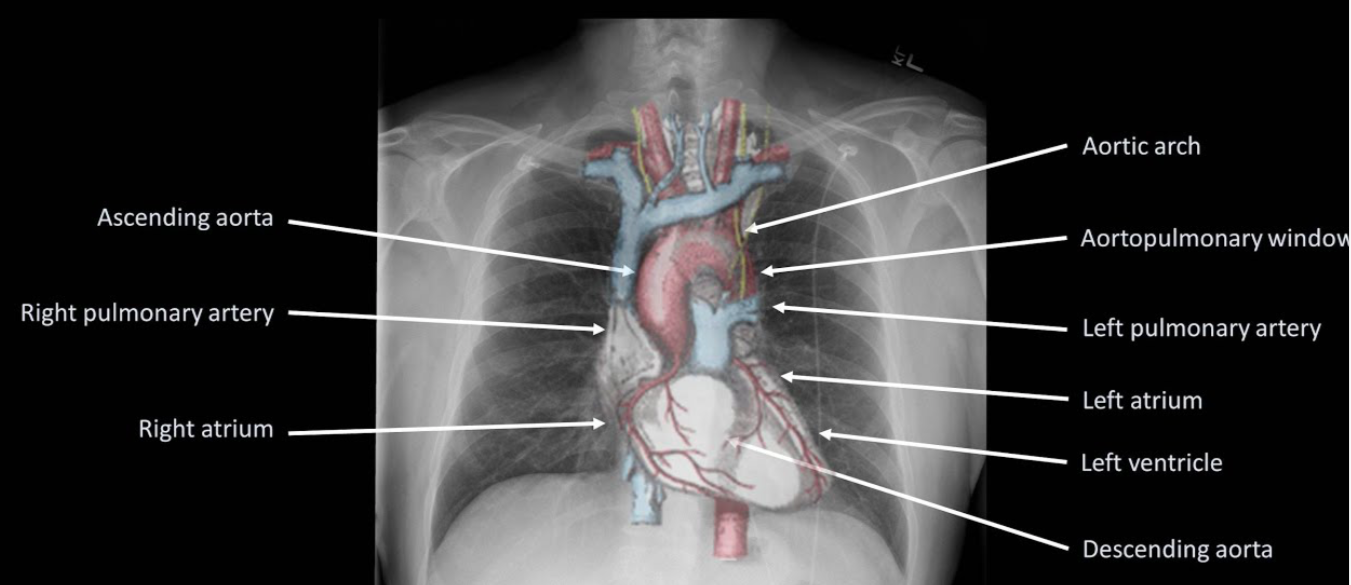
- Right heart border is formed predominantly by the right atrium along with the lower part of SVC, whilst the left border is formed by the aortic arch, pulmonary artery, left atrium, and ventricle. The right and left ventricle forms the inferior border. The right diaphragm is normally higher than the left due to the liver.
- Areas where pathology is commonly missed: Apices (including behind the 1st rib and clavicle)—small pneumothoraces and masses. Hila—masses and lymph nodes; left hilum is 1–2 cm higher than right. Behind the heart—left lower lobar collapse and hiatus hernia. Below the diaphragm—free gas. Soft tissues—breast shadow or absence (look for lung and bone metastasis)
- This is CXR of Mr Roy (Patient identity) done on 14/08/2019 (date of study)
- Its an AP film (Projection)
- Non rotated (Rotation)
- Expiratory film (Inspiratory/Expiratory)
- Adequately penetrated (Penetrated)
- Trachea is central, no foreign bodies or other abnormalities (A– Airway)
- On both sides, the bones and soft tissues appear normal; ribs, sternum, scapula, clavicle, spine, and humerus has no deposits or fractures (B-Bones and soft tissues)
- The cardiac silhoutte is normal (C-Cardiac silhoutte)
- There is no free air under the diaphragm. Bilateral costo- and cardio-phrenic angles are clear (D– Diaphragm and angles)
- No effusions. Pleura is not visible (E-Effusion)
- Both sides, the lung fields appear normal (F-Fields = lung fields)
- Gastric bubble visible at left upper abdomen (G=Gastric bubble)
- The hila and the mediastenum appears to be normal and not displaced. The CT ratio is less than 50% (H-Hila and mediastenum)
- Endotracheal tube tip is seen 5 cms above the carina or T4/T5 interspace. NG tube passed down midline, past level of diaphragm, and deviates to left with tip seen in stomach. ECG leads and electrodes are noted (I=Insertions, Interventions: tubes and lines, chest drains, pacemakers, and metallic valves and artefacts)
- If an intrathoracic opacity is in anatomical contact with the heart border, then the opacity will obscure that border. If an intrathoracic opacity is in the posterior pleural cavity so not in direct anatomical contact with the heart border, this causes an overlap but not an obliteration of that border (Silhoutte sign)
- When the alveoli no longer contain air and opacify, the air-filled bronchi passing through the alveoli may be visible as branching linear lucencies. (Air bronchogram)
- Linear opacities measuring 1–6 cm extending from periphery to the hila caused by distension of anastomotic channels between peripheral and central lymphatics.(Kerley A lines)
- Short horizontal lines, due to oedema of the interlobular septae, situated perpendicularly to the pleural surface at the lung base (Kerley B lines)
- Reticular opacities at the lung base (Kerley C lines)
- The mediastinal masses can be identified on the PA views but lateral films and/or CT scans are required to confirm further diagnosis
- Anterior mediastenum: Anterior to trachea, Middle mediastenum: Anterior to heart, Posterior mediastenum: Posterior to heart
- ANTERIOR MEDIASTENAL MASS: (4 T’s) Thymic tumour -Teratoma- Thyroid – Terrible lymph nodes (LN) Ascending aortic aneurysm, MIDDLE MEDIASTENAL MASS (BAL) Bronchogenic cyst – Arch aneurysm- LNs, POSTERIOR MEDIASTENAL MASS: as expected it can be from Spine/Neurogenic; also hiatus hernia
- Hilar mass: Most commonly TB/Sarcoidosis; also lymphoma
- Collapse: Triangular opacity, Crowding of ribs, Mediastenal displacement, hyperinflation of other lobes
- Consolidation: confluent ill defined opacity, bat wing distribution, no volume loss, air bronchogram
- Effusion: Erect: obliteration of the costo- and cardio-phrenic angles and opacity with meniscus. Supine: graded haze giving a ground glass opacity
- Emphysema: Decreased lung markings, flat diaphragm and hyperexpanded lung, Presence of bullae and peribronchial thickening, signs of cor pulmonale, right ventricular enlargement, pulmonary hypertension—enlargement of the central pulmonary arteries with oligaemic peripheral lung fields
