WHETHER TO DO C SPINE IMAGING IN TBI; CRITERIAS:
1. 
2. Under the NEXUS guidelines, when an acute blunt force injury is present, a cervical spine is deemed to not need radiological imaging if all the following criteria are met:
- There is no posterior midline cervical tenderness
- There is no evidence of intoxication
- The patient is alert and oriented to person, place, time, and event
- There is no focal neurological deficit (see focal neurological signs)
- There are no painful distracting injuries (e.g., long bone fracture)
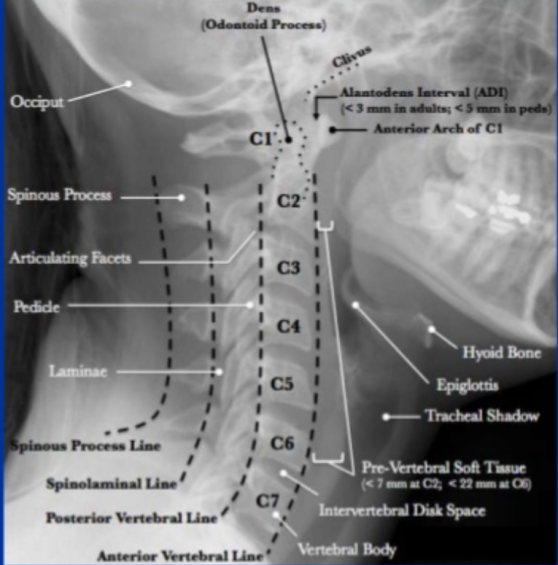
Lateral C-Spine Radiograph. (AABCDs)
A—Adequacy: An adequate film should include all seven cervical vertebrae and C7/T1 junction with optimum density so that the soft tissue shadow is visible clearly.
A—Alignment
a. Atlanto occipital alignment: The anterior and posterior margins of the foramen magnum should line up with the dens and the C1 spinolaminar line.
b. Vertebral alignment
Look for the following four lines (any incongruity= should be considered as evidence of ligamentous injury or occult fracture)
1. Anterior vertebral line—joining the anterior margin of vertebral bodies
2. Posterior vertebral line—joining the posterior margin of vertebral bodies
3. Spinolaminar line—joining the posterior margin of spinal canal
4. Spinous process/ Interspinous line—joining the tips of the spinous processes
B Bony Landmark: vertebral bodies, pedicles, laminae, and the facet joints are inspected
C Cartilagenous space: Predental space or the Atlanto-Dental Interval (ADI): which is the distance from dens to the body of C1. ADI should be < 3 mm in adults and < 5 mm in children. An increase in ADI depicts a fracture of the odontoid process or disruption of the transverse ligament
D—Disc space
Disc spaces should be roughly equal in height and symmetrical.
Loss of disc height can happen in degenerative diseases.
S—soft tissue
Prevertebral soft tissue space thickness can help in the diagnosis of retropharyngeal haemorrhage, which can be secondary to vertebral fractures. Maximum allowable distances :
Nasopharyngeal space (C1): 10 mm
Retropharyngeal space (C2–C4): 5–7 mm
Retrotracheal space (C5–C7): 14 mm in children and 22 mm in adults
