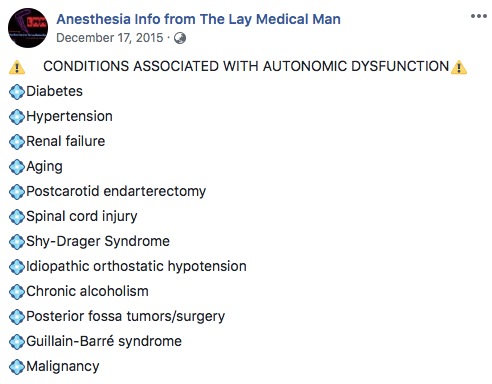
CONDITIONS ASSOCIATED WITH AUTONOMIC DYSFUNCTION
Typically affects only a segment of the hemidiaphragm
Is due to incomplete muscularisation of the diaphragm with a thin membranous sheet replacing the normal diaphragmatic muscle.
Over time this region stretches and on inspiration does not contract normally.
Sudden rupture can occur with increase in intra-abdominal pressure (e.g. coughing, straining during light anesthesia or extubation etc)
True rupture (if it happens) – Effects:
Mass effect of the abdominal viscera–>direct compression of the heart, mediastinal shift
Compression of vena cava and pulmonary veins–> impairs venous return, decreased cardiac output.
So we should maintain adequate depth of anaesthesia
Avoid Nitrous oxide (expansion of intra-abdominal viscera can impair the circulation and respiration)
Reference: Anaesthetic Management of an Adult Patient with Diaphragmatic Eventration
Azhar Rehman*, Zafar Ali Mirza, Saad Yousuf and Asma Abdus Salam

MNEMO>
Aorta is the vessel, which ‘TURNs back’
Answer: Coarctation of Aorta, Aortic Valvular Disease!!
Normal range (2.5-4.5 mg/dL),
Hypophosphataemia = phosphate concentration < 2.5 mg/dL or 0.81 mmol/L
CAUSES:
Poor Nutrition
Chronic Alcoholism
Diarrhoea
Beta 2 Agonists
Insulin Acetazolamide
Hemodialysis
Hyperparathyroidism
EFFECTS
Irritability
Confusion
Metabolic encephalopathy
Coma
Muscle weakness
Respiratory failure
Failure to wean from ventilator
Dysphagia
Ileus
cardiac arrhythmias and cardiomyopathy.
ODC shift to left
TREATMENT
Asymptomatic mild-to-moderate hypophosphatemia (1-2.5 mg/dL) can be treated with oral phosphate supplementation if the gastrointestinal tract is intact.
Symptomatic or severe hypophosphatemia (< 1.0 mg/dL) should be treated with intravenous phosphate.
Oral supplementation : 2.5 to 3.5 g (80 to 110 mmol) per day, divided over two to three doses.
Intravenous:
The required dose of initial intravenous phosphate may vary from 2.5 to 19.8 mg/kg.
Typically, 2-5 mg/kg of inorganic phosphate dissolved in 0.45% saline is given over 6-12 hours and repeated as needed.
Rapid or large infusions are dangerous : Large intravenous doses of phosphate may result in hyperphosphatemia, hypomagnesemia, hypocalcemia, and hypotension.
Hyperkalemia is prevented by using sodium phosphate instead of potassium phosphate in patients with potassium levels >4 mmol/L.
Do not mix with Calcium or Magnesium
Daily Phosphate level monitoring should be done
![]() 〰NEW INSIGHTS
〰NEW INSIGHTS![]() 〰
〰
FGF23 recently identified as a physiological regulator of phosphate and vitamin D metabolism
FGF23 plays a central role in the pathogenesis of altered mineral metabolism and secondary hyperparathyroidism in CKD patients and post-transplant hypophosphatemia in kidney transplant recipients.
FGF23 can be used not only as a biomarker for assessing phosphate retention but also as a predictor of mortality and future development of re- fractory hyperparathyroidism.
1. The evaluation of risk factors, is for planning the anesthetic management, and will be of no use in predicting the outcome.
2. There is no justification for performing revascularisation purely to facilitate elective non cardiac surgery.
3. M.I. within the last 6 weeks, class iii-iv angina, decompensated heart failure, malignant arrhythmias, severe valvular heart disease, CABG/PTCA within the last 6 weeks constitute major Cardio Vascular risk factors for surgery.
4. Previous M.I. (>6weeks), class i-ii angina, compensated heart failure, T2 DM constitute intermediate C. V. risk factors.
5. Age > 70 years, uncontrolled systemic hypertension, arrhythmias, family h/o CAD, dyslipidemia, smoking, renal dysfunction, ECG abnormalities (LVH, RBBB/LBBB, ST segment anomalies) constitute minor C. V. risk factors.
6. Only emergency, life saving procedures should be performed during the first 6 weeks after a myocardial infarction (M. I.) and after CABG/PTCA with or without a coronary stent. The period between 6 weeks and 3 months are considered as a period of intermediate risk, when non urgent elective surgery should be postponed.
7. SURGICAL PREDICTORS OF INCREASED PERIOPERATIVE CARDIOVASCULAR RISK
(i) HIGH RISK (complication rate >5%)
#Emergency major to intermediate surgery, especially in elderly patients
#Aortic & major vascular surgery; and also peripheral vascular surgery
#Procedures involving: hemodynamic instability, long duration or large fluid/blood loss
(ii) INTERMEDIATE RISK (complication rate 1-5%)
#Carotid endarterectomy
#Head & neck surgery
#Abdominal/thoracic surgery
#Orthopaedic surgery
#Prostatectomy
(iii)LOW RISK (complication rate <1%)
#Endoscopic procedure
#Breast and superficial surgery
#Eye surgery
8. ACE inhibitors are withheld for 24 hours by some anesthetists.
9. Perioperative beta blockade should be continued for 72 hours postoperatively.
10. The gold standard for detecting intraoperative ischemia and assessing volume status & valvular function is TEE.
11. Most perioperative myocardial infarctions occur in the first 3 days postoperatively. Patients at risk for M.I. require effective analgesia and humidified oxygen therapy for atleast 72 hours after major surgery.
12. Severe hypertension (grade 3) has been associated with an increased incidence of perioperative hemodynamic instability, silent m.i. and arrhythmias; but evidence of a clinically significant increase in adverse outcome is lacking. The presence of endorgan damage due to hypertension is more important than the blood pressure per se.
13. Ideally the blood pressure should be maintained within 20% of the best estimate of preoperative pressure.
14. The treatment of arrhythmias produced by WPW syndrome includes Flecainide, Disopyramide, Procainamide and Amiodarone. Digoxin and Verapamil are contraindicated.
15. There is no evidence to suggest that, frequent ventricular ectopics or asymptomatic non sustained ventricuar tachycardia is associated with an increased incidence of perioperative M.I.
16. Sick sinus syndrome is associated with a high risk of thromboemboism and may be anticoaguated. If the patient is not having a permanent pacemaker, he/she needs a, temporary pacing wire inserted preoperatively.
17. Complete heart block, type ii second degree A-V block and lesser degrees of heart block, in the presence of symptoms or cardiac failure requires preoperative insertion of permanent or temporary insertion of pacemaker. Volatile agents prolong cardiac conduction and can worsen heart block. Atropine, Isoprenaline and facilities for external pacing should be kept ready.
18. ATRIOVENTRICULAR BLOCKS
(i) First degree block: P-R interval > 0.2 sec
(ii)Second degree block
Type I: progressive lengthening of PR interval, until conduction fails and a beat is dropped.
Type II: intermittent failure of AV conduction without preceding PR prolongation.
(iii) Third degree block
Complete dissociation of atria and ventricles as atrial impulses fails to be transmitted.
19. CHECKLIST FOR A PATIENT WITH PACEMAKER
a. Indication for pacemaker insertion
b. Mode of function of pacemaker
c. Functional status
d. Consider conversion of rate responsive pacemakers to fixed rate in the perioperative period.
e. Ensure use of only bipolar diathermy
f. If unipolar diathermy must be used, then the ground plate should be placed on the same site as the operating site, as far away from the pacemaker as possible. The frequency and duration of use should be minimised and the lowest possible current used.
g. MRI is contraindicated
h. Magnets should not be placed over pacemakers during surgery, as they have an unpredictable effect on the programming of modern pacemakers.
i. A backup pacing system, atropine, adrenaline, isoprenaline and a backup pacing system should be available, in case of pacemaker failure.
20. Anesthesia constitutes a significant risk in Hypertrophic Obstructive Cardiomyopathy. Patients will be having dynamic left ventricular outflow tract obstruction, often with secondary MR. They are prone to arrhythmias and sudden cardiac death. Look for an Ejection systolic murmur in auscultation and LVH in ecg. Confirmation is by ECHO. Avoid hypovolemia, vasodilatation and the use of catecholamines
21. Constrictive pericarditis poorly tolerate vasodilatation; especially at induction.
22. In valvular heart disease, antibiotic prophylaxis is especially required for dental surgeries and those involving instrumentation of upper respiratory tract and genitourinary system.
23. AORTIC STENOSIS
# Even an ejection systolic murmur in an asymptomatic patient also warrants careful preoperative examination/ ECHO, as symptoms tend to appear late in the disease only.
# Promptly treat tachycardia and AF.
# Maintain ventricular filling by avoiding hypovolemia and maintaining SVR.
# Vasodilatation may result in profound hypotension–> subendocardial ischemia and even sudden death.
# Aggressive treatment of hypotension is mandatory to prevent cardiogenic shock and/or cardiac arrest. Cardiopulmonary resuscitation is unlikely to be effective in patients with aortic stenosis because it is difficult, if not impossible, to create an adequate stroke volume across a stenotic aortic valve with cardiac compression.
24. AORTIC REGURGITATION
# Avoid vasoconstriction and bradycardia which increases the degree of regurgitation
# A mild tachycardia, moderate fluid loading, a degree of vasodilatation and avoidence of myocardial depression can improve the forward flow.
# Acute AR is a surgical emergency and may respond poorly to vasodilatation.
25. MITRAL STENOSIS
# Patients are prone to develop CCF and Pulmonary Edema.
# Atrial fibrillation is a trigger for acute deterioration; so should be treated preoperatively
# Avoid tachycardia, myocardial depression and excessive vasodilatation
# Hypovolemia compromises ventricular filling
# Fluid overload can easily precipitate pulmonary edema
# PCWP will be inaccurate in the presence of pulmonary hyperension. Avoid Nitrous oxide if there is evidence of pulmonary hypertension.
26. MITRAL REGURGITATION
# A mild tachycardia, a slight reduction in SVR and avoidance of myocardial depression are desirable.
# Avoid hypovolemia
27. There is little evidence that GA in ADULTS with URTI is associated with an increased risk of adverse respiratory events, although upper airway reactivity may be increased
28. In children with URTI, a higher incidence of adverse respiratory events have been demonstrated, but few of these adverse events result in postoperative sequelae. It has been suggested that surgery need not necessarily be postponed in children with mild URTI. Increased airway reactivity may persist for 4-6 weeks and if surgery is postponed, it should be for a period of at least 6 weeks.
29. In COPD, if the patient is having copious secretions, better to avoid anticholinergics, as it will impair the ability to clear secretions.
30. Even though regional anesthesia has the advantage of avoiding respiratory complications of GA, most patients, even those with quite severe COPD may be managed safely under carefully conducted GA.
31. Pressure Controlled Ventilation with a low respiratory rate and prolonged expiratory phase is suitable in COPD patients.
32. Epidural analgesia has been shown to decrease the incidence of postoperative pulmonary complications in thoracic and upper abdomnal surgery.
33. In patients with bronchial asthma, good depth of anesthesia, good muscle relaxation and i. v. Lidocaine can reduce the incidence of bronchospasm during intubation; topical lidocaine spray is not effective and may induce bronchoconstriction in some patients.
34. Circulatory disturbance during anesthesia and surgery may affect the absorption of subcutaneous insulin.
>Sensitive to muscle relaxants
>Autonomic hyperreflexia , Avoid suxamethonium
>Bulbar palsy
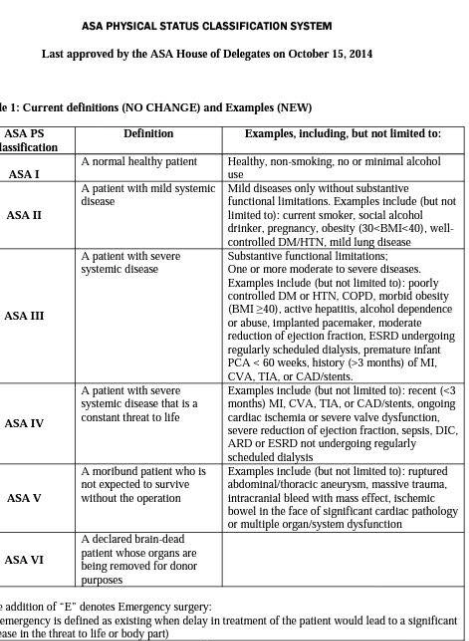
DO YOU KNOW?
A social drinker is ASA II
A smoker is ASA II
Pregnant patient is ASA II
Obese patient is ASA II
Morbid obesity is not ASA II, but ASA III
Alcohol dependence without any documented systemic illness is also ASA III
Premature infant is ASA III
ESRD with regular HD is ASA III
ESRD without regular HD is ASA IV
Evidence of Sepsis or DIC- ASA IV
Intracranial bleed with mass effect is ASA V
A cardiac patient with bowel ischemia is ASA V
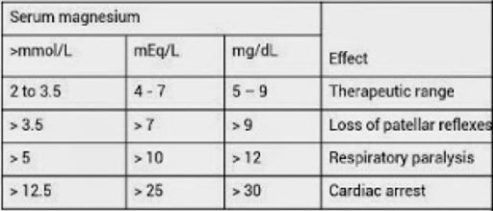
Continuous Intravenous Infusion
Magnesium sulfate 4-g to 6-g loading dose diluted in 100 mL fluid administered intravenously over 15 minutes, followed by continuous intravenous infusion at 1 to 2 g per hour. Discontinue 24 hours after delivery or last seizure.
If convulsions persist after 15 min, give up to 2 gram more intravenously as a 20% solution at a rate not to exceed 1g/min. If the patient weighs >70 kg then an additional 2 grams may be given slowly
Only give the next IM dose, or only continue the IV infusion if:
Respiratory rate > 16/min
Urine output > 25 ml/h
Patellar reflexes are present
If urine output < 100 ml in 4 h and there are no other signs of magnesium toxicity, reduce the IV infusion to 0.5 g/h.
If patellar reflexes are depressed and respiration is normal, withhold further doses of magnesium sulfate until the reflexes return and request magnesium level.
If there is concern about respiratory depression , stop magnesium, give oxygen by mask and give:
Calcium gluconate (10mL of 10% solution over 10 minutes)
ACOG TASK FORCE 2013
… For women with severe preeclampsia, the administration of intrapartum and postpartum magnesium sulfate to prevent eclampsia is recommended. For women with preeclampsia undergoing cesarean delivery, the continued intraoperative administration of parenteral magnesium sulfate to prevent eclampsia is recommended.
ANESTHETIC CONCERNS
1. Short trachea with 15 rings or less; high chance of accidental one lung ventilation
2. Chances of Laryngeal Stenosis… Some times an unanticipated difficulty for passing tube, may trigger edema and stridor
3. Atlanto axial instability, can cause, massive cord edema, even with moderate neck flexion. Take LATERAL CERVICAL SPINE VIEWS IN FLEXION AND EXTENSION PREOPERATIVELY. If atlantoaxial instability is present and patient requires GA, give MANUAL IN LINE STABILIZATION/ do AWAKE FOB.
4. Restricted lung function accompanied by impending respiratory failure, is a situation, where we may be more inclined towards SAB in such patients (e.g. Pregnancy, where the uterus further compromise lung function). So regional anesthesia may be appropriate, if technically feasible.
5. Technical difficulties with SAB/EDB; epidural space located 2.5 cm from skin was reported in one case.
This is the most frequently occurring demyelinating neuromuscular disorder. It’s a chronic progressive disease characterized by repeated exacerbations and partial remissions. It is characterized by the formation of plaques within the brain and spinal cord. These plaques cause demyelination around the axons, resulting in weakness and spasticity as well as sensory dysfunction.Upper motor neurone lesions, cerebellar lesions and sensory deficits are common.
Anaesthetic considerations.
Regional blockade.
Temperature maintenance is important as symptoms can deteriorate with an increase in temperature, as demyelinated axons are also more sensitive to heat.
Most often, postop exacerbation, if it occurs, is due to fever and infections
We should explain the chance of exacerbation of symptoms before any form of regional anesthesia
TREATMENT
The treatment of MS includes treating acute attacks to limit sequelae, prophylactic medications to reduce rate of progression, and symptomatic/supportive therapy
Acute attacks are treated with high-dose corticosteroids, i.v. methylprednisolone 500–1000 mg every day divided every 6 or 12 hours; tapered over 7–10 days.
Prophylactic medications include the disease-modifying drugs interferon β and glatiramer acetate. Side effects include local infections, fatigue, depression, and anxiety. Regular CBC, LFT, and electrolyte checks are needed.
For progressive disease, immunomodulatory drugs such as methotrexate, cyclosporine, cyclophosphamide, azathioprine, total lymphoid irradiation, mitoxantrone (risk of cardiotoxicity), mycophenolate mofetil, or interferon-β may be employed
Symptomatic therapies include antidepressants for depression, anticholinergics for hyperreflexic bladder, alpha-blockers or cholinergics/catherization for flaccid bladder, amantadine for fatigue, antispasticity drugs (baclofen, tinzanidine, dantrolene, benzodiazepines) for muscle spasticity, AEDs for tremor, clonus, and pain, and sildenafil for sexual dysfunction. More invasive methods, for example, botulinum toxin injections for focal spasticity or bladder augmentation for spastic bladder may be required in more severe cases
Supportive care includes physical/occupational therapy, coping strategies or lifestyle modifications, cognitive-behavioral therapy, and emotional support.
In more severe cases, ambulatory aids or wheelchairs and other home-assist devices and caregiver support may be necessary
