 Cranial nerves V,VII,IX,X,XI,XII contributes
Cranial nerves V,VII,IX,X,XI,XII contributes- 2 brain stem nuclei control swallowing: (1) Nucleus Tractus Solitarius(NTS) which is a pure sensory nucleus in the medulla (2) Nucleus Ambiguous (NA) which is a motor nucleus situated deep in the reticular formation in medulla
- Sensory info sent via cranial nerves to NTS. Interneurons relay info to NA & surrounding reticular formation which sends efferent messages to cranial nerve pathways.
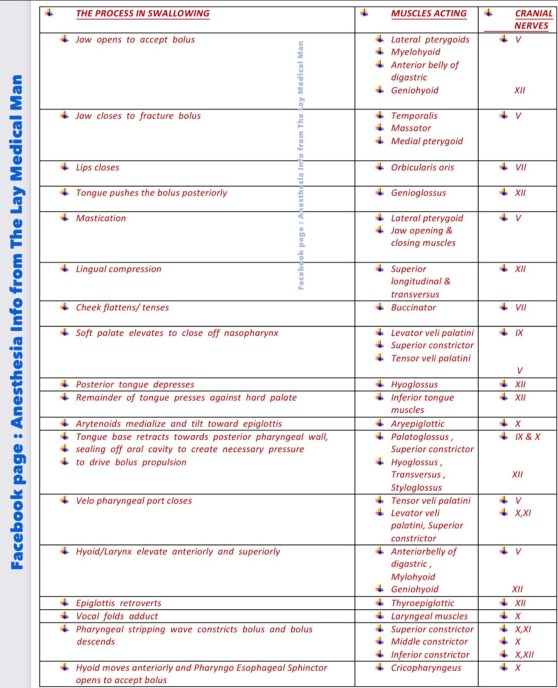
- Muscles innervated by Trigeminal nerve helps in Mastication, jaw closure, upward movement of larynx, backward movement of tongue to soft palate, tensing and elevation of soft palate and posterior pharyngeal wall constriction
- Muscles innervated by Facial nerve helps in mandibular depression and contributes to hyoid elevation
- Glossopharyngeal nerve supplies Stylopharyngeus , contributes to palatoglossus – portion of middle pharyngeal constrictor Ⓜ️NEMO> “Glossy nerve helps Stylish Middle Class”
- Vagus supplies muscles of soft palate (except Tensor Veli Palatini) – Superior, middle and inferior pharyngeal constrictors – Intrinsic muscles of larynx and muscles of esophagus Ⓜ️NEMO> “Vague nerve helps all classes”
- Recurrent Laryngeal Nerve innervates Cricopharyngeus muscle.
- Hypoglossal nerve innervates all intrinsic and some extrinsic muscles of tongue and geniohyoid ; hence responsible for all movements of the tongue
- Aetiology of swallowing disorders: Stroke, Traumatic Brain Injury, Brain Tumor , Cerebral Palsy, Neuroleptic drug- induced Tardive dyskinesia , Surgery ( Generally damage to the pharyngeal plexus may occur with anterior cervical fusion. Injury of the seventh, tenth, and twelfth cranial nerves may occur with carotid endarterectomy (as these nerves are close to the carotid bifurcation), various forms of dementia, Movement disorders including Parkinsons disease, Multiple Sclerosis , Amyotrophic Lateral Sclerosis (ALS)
- It has been suggested that recovery of swallowing in acute stroke patients may be rapid, warranting reassessment within 3 weeks of the initial swallowing evaluation
- Abnormal volitional cough, abnormal gag,dysarthria,dysphonia, cough after swallow, voice change after swallow are indicators of risk of aspiration after acute stroke
- But many of the neurologic disorders that affect swallowing are progressive; thus swallowing can be expected to decline as the disease worsens.
- Dysarthria may correlate with dysphagia with bulbar Amyotrophic Lateral Sclerosis (ALS). Dysphagia increases as respiratory capacity decreases regardless of the form of ALS. Vital capacity should be consistently measured, as accurate and timely assessment of a clinically relevant decline in respiratory status is crucial for determining the timing of feeding tube placement
- Pneumonia can be a frequent complication in patients with dysphagia owing to CNS disease
- Although an abnormal gag reflex may be apparent in patients with dysphagia resulting from various neurologic disorders, it may be absent in healthy control subjects or it may be normal in patients with neurogenic dysphagia
- The two imaging tools used to evaluate oropharyngeal dysphagia are Video Fluoroscopic Swallow Study (VSS- Gold Standard) and videoendoscopy. The Penetration-Aspiration Scale (PAS) provides an objective way during the VSS to measure the depth, response, and clearance of material entering the larynx and trachea.
- They are also valuable in identifying and teaching maneuvers that may facilitate swallowing and prevent aspiration in a patient.
- When significant aspiration cannot be prevented, alternatives to oral feeding such as percutaneous endoscopic gastrostomy (PEG) tube placement should be considered.
- Patients with oropharyngeal dysphagia owing to CNS lesions are best managed by a team approach including a speech pathologist, neurologist, and gastroenterologist.
- Swallowing therapy may include compensatory or rehabilitative strategies. Compensatory therapy does not change the physiology of the swallow; rather, bolus flow is redirected
- Compensatory strategies consist of manipulation of posture, consistency of the liquid, and sensory input. Facilitatory postures that have been studied in the neurogenic population include chin tuck and head rotation to the weak side
- Rehabilitative therapy includes muscular strengthening and range of motion exercises, thermal-tactile application, and swallowing maneuvers
- Vocal fold medialization is the procedure generally performed to treat aspiration owing to an incompetent larynx
- A tracheotomy may be performed for neurologic patients with chronic aspiration. Although it does not improve swallowing, it facilitates pulmonary toileting
- Laryngotracheal separation is a more radical attempt to prevent chronic aspiration while allowing for oral intake. Although patients may return to oral diets, the ability to phonate is eliminated. If physiologic aspects of swallowing improve sufficiently, this procedure can be reversed, as the glottis is not affected.
Category Archives: Anesthesia

#EPINEPHRINE ( #Adrenaline) : Pharmacological Highlights
🔻Epinephrine is an agonist of alpha 1, β1 , and β2 adrenoceptors. An intravenous infusion of epinephrine produces an increase in mean arterial pressure (MAP) characterized by selectively enhanced systolic pressure with no change in diastolic pressure.
🔻Epinephrine exerts positive chronotropic and inotropic actions by stimulation of β1 adrenoceptors
🔻Epinephrine also increases the rate of myocardial relaxation and enhances early LV filling, thereby improving diastolic function. These combined effects result in a dramatic increase in cardiac output.
🔻Epinephrine (0.01–0.03 ug kg –1 min –1 ) has been shown to produce similar hemodynamic effects with less pronounced tachycardia than dobutamine (2.5–5.0 ug kg–1 min–1 ) in patients after coronary artery bypass graft (CABG) surgery
🔻Predictable increase in cardiac output, favours the use of epinephrine as the primary inotropic drug for the management of LV dysfunction after cardiopulmonary bypass
🔻Epinephrine causes direct positive dromotropic effects ( leading to increase in conduction velocity and reduction of the refractory period of the AV node, His bundle, Purkinje fibers, and ventricular muscle)
🔻This may contribute to detrimental increases in ventricular rate in patients with atrial flutter or fibrillation and the occurrence of ventricular arrhythmias
🔻The overall effect of epinephrine on blood flow to a specific organ depends on the relative balance of alpha 1 and β2 adrenoceptors located in the vasculature.
🔻β2 -Adrenoceptors are sensitive to lower doses of epinephrine and, as a result, peripheral vasodilation and modest reductions in arterial pressure are observed with such doses
🔻In contrast, the effects of epinephrine on alpha 1 -adrenoceptors predominate at greater doses with marked increases in systemic vascular resistance and arterial pressure.
🔻The intense vasoconstriction produced by high doses of epinephrine may adversely impede LV ejection by increasing after load after cardiopulmonary bypass. Thus, greater doses of epinephrine may be used in combination with arterial vasodilators such as sodium nitroprusside to optimize contractile performance in such situations .
🔻Adrenaline via alpha 1 receptors also mediates (1) venoconstriction & enhanced venous return (2) Pulmonary vasoconstriction and increases in pulmonary arterial pressures.
🔻 Pre-existing β-blockade by nonselective β-blocker propranolol abolishes the decrease in systemic vascular resistance from epinephrine-induced stimulation of β2 adrenoceptors and potentiates peripheral vasoconstriction mediated by unopposed alpha 1 adrenoceptors.
🔻The positive inotropic and chronotropic effects of epinephrine are also attenuated in the presence of pre-existing β-blockade and greater doses of epinephrine are required to overcome this competitive blockade
🔻Complete pharmacologic blockade of β1 and β2 adrenoceptors may theoretically make the hemodynamic effects of epinephrine indistinguishable from those of the pure alpha 1 adrenoceptor agonist phenylephrine.
#NorAdrenaline , #CriticalCare , #vasopressors , #TheLayMedicalMan , #IntensiveCare , #Pharmacology, #anesthesia , #anaesthesia, #drugs
(Reference: Paul S. Pagel and David C. Warltier, Essential drugs in anesthesia practice Positive inotropic drugs, Anesthetic Pharmacology, 2nd edition)
JNC 8 GUIDELINES FOR MANAGEMENT OF SYSTEMIC HYPERTENSION
(1)📌In the general population aged 60 years or more , initiate pharmacologic treatment to lower blood pressure (BP) at systolic blood pressure (SBP) ≥150 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg and treat to a goal SBP <150 mm Hg and goal DBP <90 mm Hg
(2)📌In the general population aged ≥60 years, if pharmacologic treatment for high BP results in lower achieved SBP (eg, <140 mm Hg) and treatment is well tolerated and without adverse effects on health or quality of life, treatment does not need to be adjusted.
(3)📌In the general population <60 years, initiate pharmacologic treatment
(a) to lower BP at DBP ≥90mmHg and treat to a goal DBP <90mmHg.
(b) to lower BP at SBP ≥140 mm Hg and treat to a goal SBP <140 mm Hg.
(4)📌In the population aged ≥18 years with (i) diabetes & (ii) chronic kidney disease (CKD), initiate pharmacologic treatment to lower BP at SBP ≥140 mmHg or DBP ≥90 mmHg and treat to goal SBP <140mmHg and goal DBP <90mmHg.
(5)📌In the general nonblack population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic, calcium channel blocker (CCB), angiotensin-converting enzyme inhibitor
(ACEI), or angiotensin receptor blocker (ARB).
(6)📌In the general black population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic or CCB.
(7)📌In the population aged 18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race
or diabetes status.
(8)📌If goal BP is not reached within a month of treatment, increase the dose of the initial drug or add a second drug from one of the classes : thiazide-type diuretic, CCB,ACEI, or ARB. The clinician should continue to assess BP and adjust the treatment regimen until goal BP is reached.
(9)📌If goal BP cannot be reached with 2 drugs, add and titrate a third drug from the list mentioned above (). Do not use an ACEI and an ARB together in the same patient.
(10)📌If goal BP cannot be reached using only the drugs mentioned above, because of a contraindication or the need to use more than 3 drugs to reach goal BP, antihypertensive drugs from other classes can be used.
#hypertension , #medicine , #TheLayMedicalMan , #jnc8 , #HTN , #anesthesia , #pharmacology , #BloodPressure ,#BP
NORADRENALINE: PHARMACOLOGICAL HIGHLIGHTS & COMPARISON WITH ADRENALINE
Noradrenaline (Norepinephrine) is a directly and indirectly acting sympathomimetic amine which stimulates alpha 1 and β1 adrenoceptors, but, in contrast to Adrenaline (epinephrine), has little effect on β2 adrenoceptors.
🖍These actions produce positive inotropic effects, intense vasoconstriction, increases in arterial pressure, and relative maintenance of cardiac output.
🖍Noradrenaline increases arterial pressure while simultaneously enhancing contractile state and venous return by reductions in venous capacitance, thereby augmenting stroke volume and ejection fraction. In contrast, pure alpha 1 adrenoceptor agonists such as phenylephrine and methoxamine further compromise cardiac output in failing myocardium and contribute to peripheral hypoperfusion despite an increase in arterial pressure.
🖍In contrast to adrenaline, noradrenaline does not substantially affect heart rate because activation of baroreceptor reflexes resulting from arterial vasoconstriction usually counteracts β1 mediated, direct, positive, chronotropic effects.
🖍Its arrhythmogenic potential is considerably less than that of adrenaline. Thus, substitution of noradrenaline for adrenaline may be appropriate in the therapeutic management of cardiogenic shock when atrial or ventricular arrhythmias are present.
🖍Intravenous infusions of noradrenaline (0.03–0.90 mg kg –1 per minute) have been shown to increase arterial pressure, LV stroke work index, cardiac index, and urine output in septic patients with hypotension that was unresponsive to volume administration, dopamine or dobutamine
🖍Causes relatively greater increases in systemic vascular resistance and diastolic arterial pressure than adrenaline.
🖍The drug has a duration of action of 30–40 minutes; tachyphylaxis occurs with prolonged administration.
🖍The drug produces coronary vasodilatation, leading to a marked increase in coronary blood flow. However, as myocardial work may increase, the balance of myocardial oxygen consumption and delivery may lead to ischaemia on noradrenaline.
🖍Reflex vagal stimulation leads to a compensatory bradycardia
🖍The cerebral blood flow and oxygen consumption are decreased by the administration of noradrenaline; mydriasis also occurs
🖍The glomerular filtration rate is usually well maintained with noradrenaline; but it decreases the renal blood flow and this represents a major limitation on the prolonged use of high doses of norepinephrine.
🖍Noradrenaline increases the contractility of the pregnant uterus; this may lead to fetal bradycardia and asphyxia
🖍Noradrenaline may decrease insulin secretion, leading to hyperglycaemia
🖍The drug is pharmaceutically incompatible with barbiturates and sodium bicarbonate
(Reference: Paul S. Pagel and David C. Warltier, Essential drugs in anesthesia practice Positive inotropic drugs, Anesthetic Pharmacology, 2nd edition)
Transurethral resection of the prostate (#TURP) syndrome : A summary
🚩#TURPsyndrome is diagnosed based on clinical signs, symptoms and biochemical findings
🚩The manifestations are due to hypervolemia, hyponatremia and due to the direct toxicity of the irrigation fluids like 1.5% glycine
▪️FACTORS INCREASING THE ABSORPTION OF THE IRRIGATION FLUID ( AND THUS CONTRIBUTING TO THE HYPERVOLEMIA )
🚩Long duration of the surgery: the irrigation fluid is absorbed at the rate of 20-30 mL/ min and so the volume absorbed increases with the duration of the surgery
🚩High pressure delivery of the irrigation fluid especially from a considerable height; the minimum height required for adequate flow should be used (usually 70 cms)
🚩Low venous pressures
🚩Excessive bleeding (= there are more open veins)
🚩Large prostate (>50g)
▪️CLINICAL FEATURES:
🚩Headache, Restlessness, Agitation, Confusion, Convulsions, Coma; pulmonary oedema may also set in. If patient is under general anesthesia, these symptoms will get masked.
▪️MANAGEMENT FROM SURGICAL SIDE:
🚩Coagulating bleeding points and terminating surgery as soon as possible.
▪️ANESTHETIC MANAGEMENT:
🚩Reduce / stop fluid administration. Diuretics may be required in the presence of pulmonary oedema
🚩Intubation to protect the airway and mechanical ventilation to support respiration may be required
🚩Anti-convulsants, if needed, to treat seizures
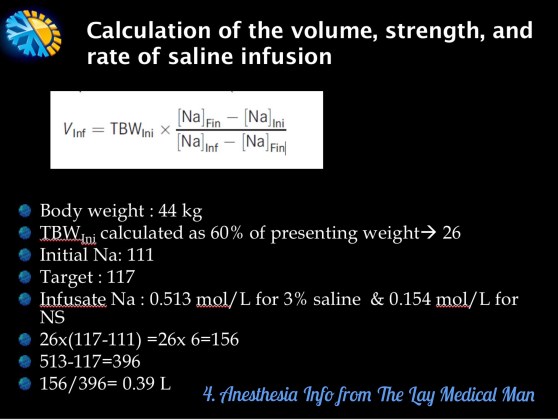
🚩Hypertonic saline should be considered for severe hyponatremia (<120 mmol L−1) or in the presence of severe neurological symptoms.
👉🏿N.B.- Central pontine myelinolysis or osmotic demyelinating syndrome (ODS) is more likely to occur with correction of serum Na greater than 8-12 mmol/day and in the setting of chronic hyponatremia (greater than 48 h)
👉🏿Faster rates of administration can potentially lead to central pontine myelinolysis. Treatment should stop once symptoms have resolved or the serum sodium is more than 125 mmol L−1. Such therapy is best delivered in a high-dependency environment.
🔻A template is given below for calculating the volume of hypertonic saline
#anesthesia , #urology ,#hyponatremia , #anaesthesiologist

VIVA AID: BISPECTRAL INDEX
💆The EEG bispectrum is a high-order statistical computation derived from the analog EEG.
💆The BIS is a combination of three weighted parameters: (i) the burst suppression ratio (the proportion of isoelectric EEG signal in an epoch); (ii) the beta ratio (a measure of the proportion of signal power in the high vs medium frequency range); and (iii) the SynchFastSlow (relative synchrony of fast and slow waves)
💆Changes in frequency and power alone ( as done with conventional power spectral analysis) have been shown to be inconsistent when attempting to measure anesthetic depth.
💆Bispectral analysis incorporates information on power and frequency with the phase coupling information that is more indicative of anesthetic depth but not present in other clinical applications of EEG.
💆The BIS uses a combination of EEG subparameters that were selected after analysis of a large database of EEGs to demonstrate specific ranges for varying phases of anesthetic effect
💆These parameters were then combined to form the optimum configuration for monitoring of the hypnotic state.
💆The BIS is then displayed as a dimensionless number between 0 and 100 with the lower numbers corresponding to deeper levels of hypnosis.
💆There are normal, genetically determined low-voltage EEG variants among the population that can result in abnormally low BIS values in awake patients; therefore, it is important to obtain baseline values before the induction of anesthesia
💆BIS is not able to predict movement in response to surgical stimulation because the generation of reflexes is likely to be at spinal cord rather than cortical level
💆BIS does not fully reflect the synergistic effect of opioids with hypnotic agents
💆The presence of electromyographic artefacts, poor signal quality, and electrical artefacts such as those from electro-cautery and forced air warming units can cause spurious values to be displayed by the BIS monitor.
💆With the administration of ketamine, the BIS may remain high, possibly due to the excitatory actions of ketamine, and, therefore, the BIS monitor is not reliable when used to monitor hypnosis with ketamine.
💆There have been studies in which the BIS monitor has not been shown to reflect the hypnotic contribution to the anesthetic by nitrous oxide.
💆Potential benefits from the routine use of the BIS monitor include
➖decreased risk of awareness
➖improved titration of anesthetic agents and
➖decreased recovery room time
💆The BIS also gives the anesthetist additional information to consider when selecting drugs for interventions, for example, when making the decision whether to deepen anesthesia with a volatile agent, add more analgesia with an opioid, or use a vasoactive drug.
💆Also note:
➖The BIS may drop after giving a neuromuscular blocking agent if excessive EMG was present prior to giving it.
➖Ischemia attenuates the amplitude and frequency of the EEG signal, which may result in a decrease in BIS
➖Hypothermia decreases brain activity, and may decrease BIS
➖Muscle shivering, tightening, twitching etc may increase EMG and increase BIS
➖Artifacts in the higher frequency ranges [e.g. use of any mechanical device that could generate high frequency activity like patient warmer]can artificially increase the BIS value
➖Is the BIS decreasing when you think it should be increasing? Think of Paradoxical Delta pattern (characterized by a pronounced slowing of the EEG) which occurs over a short period of time (2-3 minutes).
➖If the sensor is placed over the temporal artery, pulse artifacts can cause the BIS value to be inappropriately low. Check EEG waveform for presence of pulse artifacts and move sensor if necessary.
➖Blinking or rolling his/her head by the patient, may cause artifacts that mimic slow frequency EEG patterns.
Reference: The BIS monitor: A review and technology assessment, James W. Bard, AANA Journal/December 2001/Vol. 69, No. 6
A FEW PROSPECTIVE TECHNIQUES TO MEASURE ANALGESIA INTRA-OPERATIVELY
🤖Current electroencephalogram (EEG)-derived measures like BIS, provide information on cortical activity and hypnosis but are less accurate regarding subcortical activity, which is expected to vary with the degree of antinociception.
🤖Efforts to develop methods for monitoring these subcortical activities produced a few indices, which may provide some use intra-operatively
🤖Recently, the neurophysiologically based EEG measures of cortical input (CI) and cortical state (CS) have been shown to be prospective indicators of analgesia/anti-nociception and hypnosis, respectively. Composite Cortical State (CCS) is an alternate measure of CS.
🤖Composite Variability Index (CVI) is another recently developed EEG-derived measure of antinociception based on a weighted combination of BIS and estimated electromyographic activity.
🤖CCS and BIS show strong correlations, suggesting that they behave similarly as indicators of hypnosis.
Reference: Comparisons of Electroencephalographically Derived Measures of Hypnosis and Antinociception in Response to Standardized Stimuli During Target-Controlled
Propofol-Remifentanil Anesthesia, Mehrnaz Shoushtarian, Marko M. Sahinovic, Anthony R. Absalom, Alain F. Kalmar, Hugo E. M. Vereecke, David T. J. Liley and Michel M. R. F. Struys, anesthesia-analgesia, February 2016 • Volume 122 • Number 2
WHAT IS SURGICAL STRESS INDEX (SSI)❓
🔵 SSI is an index which measures the surgical stress response in patients under anesthesia
🔵 It assess the balance between the intensity of surgical stimulation and the level of antinociception (e.g. Opioid analgesia , neuraxial or nerve blockade)
🔵 SSI uses two continuous cardiovascular variables, both obtained from Photo Plethysmography (PPG) waveforms of SpO2
(1) The interval between successive hearts beats (HBI)
(2) PPG amplitude (PPGA)
🔵Photoplethysmography (PPG), i.e. pulse oximetry, is primarily used to produce an estimation of the relative concentration of oxyhemoglobin in blood.
🔵 PPG is related to volume changes and contains information about the peripheral blood circulation, including skin vasomotion. Skin vasomotion is controlled by the sympathetic nervous system, which is activated during surgical stress.
🔵 Changes in PPG amplitude (PPGA) reflect changes in the peripheral vascular bed, controlled by the sympathetic nervous system . Increased PPGA response has been associated with nociception during general anesthesia.
🔵SSI values near 100 correspond to a high stress level, and values near zero to a low stress level.
🔵 In trials, SSI correlated positively with the intensity of painful stimuli and negatively with the analgesic concentration
🔵 SSI has been shown to be capable of differentiating decreases in HR achieved with opioid from those accomplished with a beta blocker (Ahonen et al. 2007).
🔵 An optimal range for SSI during anesthesia has not yet been recommended.
Reference: Measurements of adequacy of anesthesia and level of consciousness during surgery and intensive care, Johanna Wennervirta, Department of Anesthesiology and Intensive Care Medicine, Helsinki University Hospital
#anaesthesia , #anaesthesiology , #anaesthesiologist
👁➖BE AWARE OF AWARENESS ➖👁
💣Premedication with amnestic reduces the chance of awareness. Also, if awareness occurs, psychological trauma is less likely without recall.
💣Light induction doses and liberal use of muscle relaxants ,without giving adequate concern to the depth of anaesthesia can increase the chance of awareness.
💣Better to give re-bolus with i.v. hypnotic during multiple intubation attempts. Consider using inhalation induction technique.
💣Beta-blockers, can reduce MAC-Awake and may also decrease the likelihood of PTSD.
💣We can consider ear plugs or headphones to reduce awareness of noises in the OR.
💣Nitrous oxide, Ketamine and Opioids suppress cortical arousal during painful stimulation, which may reduce the probability of awareness. But BIS (Bi Spectral Index) and other EEG monitors do not accurately predict the depth of anesthesia with these drugs. (Because, even though they produce hypnosis, they do not modulate GABA-A receptors and are associated with unchanged or increased high frequency EEG signals.)
💣Propofol, barbiturates, etomidate, and halogenated volatile anesthetic agents all modulate GABA-A receptor activity and shift the cortical EEG to lower frequencies. So, BIS and other EEG-based monitors provide strong correlation with hypnosis for this group of general anesthetics.
💣MAC for N2O & volatile anesthetics is additive (i.e. a mixture of 0.5 MAC N2O plus 0.5 MAC volatile suppresses movement in response to pain like 1 MAC volatile. The HYPNOTIC activities of nitrous oxide and volatile anesthetics are sub-additive. (i.e. a mixture of 0.5 MAC-awake N2O + 0.5 MAC-awake volatile anesthetic is not as hypnotic as 1 MAC-awake volatile. This suggests that N2O has an action which antagonizes the hypnosis induced by volatile anesthetics, perhaps via direct cortical arousal.
💣Many studies say, BIS is not useful in case of dexmedetomidine also; while some others say it will help.
#awareness , #anesthesia , #sedation , #AwarenessAnesthesia , #bis , #AwarenessSurgery
➖➖➖➖➖➖➖➖➖➖➖➖➖➖➖➖➖➖
Reference:
CampagnaJA,MillerKW,FormanSA:Mechanismsofactionsof inhaled anesthetics. N Engl J Med 348:2110-2124, 2003
SleighJW,BarnardJP:Entropyisblindtonitrousoxide.Canwesee why? Br J Anaesth 92:159-161, 2004 39.
ChortkoffBS,BennettHL,EgerEI2nd:Doesnitrousoxideantagonize isoflurane-induced suppression of learning? Anesthesiology 79: 724-732, 1993 40.
KatohT,IkedaK,BitoH:Doesnitrousoxideantagonizesevofluraneinduced hypnosis? Br J Anaesth 79:465-468, 1997
Update on Bispectral Index monitoring Jay W. Johansen,Best Practice & Research Clinical Anaesthesiology Volume 20, Issue 1, March 2006, Pages 81–99
EXPLICIT AND IMPLICIT AWARENESS DURING ANESTHESIA
😐(Explicit = Fully and clearly expressed)
😐(Implicit =Implied or understood though not directly expressed)
😐The incidence of awareness is around 0.1–0.2%
😐Explicit Awareness is intentional or conscious recollection of prior experiences as assessed by tests or recall or recognition, which are also called direct memory test.
😐Implicit Awareness is perception without conscious recall. The patient denies recall, but may remember “something” under hypnosis.
😐Awareness (deliberate)
Surgery conducted under local or regional anaesthesia. During some neurosurgical procedures, the patient is woken up to assess whether surgery has affected, or will affect, important areas.
😐STAGES OF AWARENESS ( Griffith and Jones )
1. Conscious perception with explicit memory;
2. Conscious perception without explicit memory;
3. Dreaming;
4. Subconscious perception with implicit memory;
5. No perception and no implicit memory.
😐CAUSES
🔻may result from a failure of the apparatus to deliver adequate concentrations of anesthetic agent. Such failures include leaks, faulty or empty vaporizers, a misconnected or disconnected breathing system, inaccurate pumps, misplaced venous cannula and occluded infusion tubing
🔻failure of the clinician to monitor the concentrations of inspired and expired volatile agents may result in inadequate anesthetic agent being delivered. TIVA is more difficult to monitor in this respect.
🔻may result from an inadequate dosing of the anesthetic agent as represented by the alveolar concentration (it is important to remember that the MAC value that is quoted is only the MAC 50 ) or the computed blood concentration in target-controlled infusion (TCI).
🔻may result from an altered physiology or pharmacodynamics in the patient e.g. Anxiety may increase dose requirements
🔻may result from the wearing off of the induction agent during a difficult intubation sequence or with the anesthetic techniques for rigid bronchoscopy
😐CLINICAL SIGNS
🔻In the spontaneously breathing patient who is not paralyzed, awareness may be manifest by purposeful movement.
🔻Sympathetic stimulation: the main clinical signs are tachycardia, hypertension, diaphoresis and lacrimation; but their absence does not exclude awareness. Attempts have been made to quantify these objectively by using the PRST scoring system (blood Pressure, heart Rate, Sweating, Tear formation)..
😐SEQUELAE:
Commonest is the occurrence of a post-traumatic stress syndrome, whose typical features may include nightmares, insomnia, panic attacks and agoraphobia.
😐CHECKLIST FOLLOWING A COMPLAINT OF AWARENESS DURING GENERAL ANAESTHESIA
1. Visit the patient as soon as possible, along with a witness (Preferably a consultant)
2. Take a full history and document the patient’s exact memory of events
3. Attempt to confirm the validity of the account
4. Keep your own copy of the account
5. Give a full explanation to the patient
6. Offer the patient follow-up, including psychological support, and document that this has been offered
7. Reassure the patient that they can safely have further general anaesthetics, with minimal risk of a further episode of awareness
8. If the cause is not known, try to determine it
9. Notify your medical defence organisation
10. Notify your hospital administration
11. Notify the patient’s GP
#awareness , #ptsd , #AnesthesiaComplications , #TheLayMedicalMan , From http://www.facebook.com/drunnikrishnanz , partial reference from frca.uk , #anaesthesia
