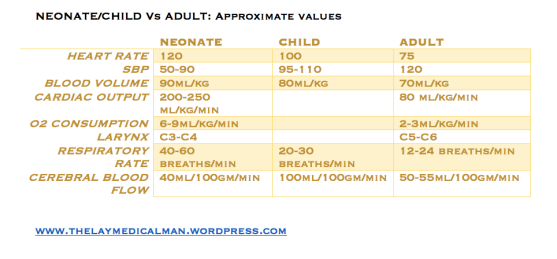
CHILD Vs ADULT; Numericals
The inspiratory positive airway pressure (IPAP) is similar to the peak airway pressure in traditional mechanical ventilation. A higher IPAP level would result in a larger tidal volume and minute ventilation.
The expiratory positive airway pressure (EPAP) is the same as PEEP during mechanical ventilation or CPAP during spontaneous breathing. In addition to its ability to improve oxygenation by increasing the functional residual capacity, EPAP also relieves upper airway obstruction with its splinting action.
SpO2, Capnography, PaO2, PaCO2 etc may be used for the titration of appropriate IPAP and EPAP levels.
CPAP (Continuous positive airway pressure) provides positive airway pressure during spontaneous breaths and it does not include any mechanical breaths. For this reason, the work of breathing is entirely assumed by the patient. CPAP is active when IPAP=EPAP. CPAP is the treatment of choice for obstructive sleep apnea without significant carbon dioxide retention. CPAP should not be used in apnea due to neuromuscular causes, if there is progressive hypoventilation or facial trauma
Bilevel PAP (Bilevel positive airway pressure) provides IPAP which controls peak inspiratory pressure during inspiration and EPAP that controls end-expiratory pressure. Indications are acute respiratory failure and acute hypercapnic exacerbations of COPD
In patients with acute cardiogenic pulmonary edema, CPAP or bilevel PAP ventilation has been found to reduce the need for subsequent mechanical ventilation
Inability to protect the airway from secretions or aspiration, apnoea, facial trauma are contraindications for NPPV.
Subcutaneous emphysema, refers to gas in the subcutaneous tissues
Clinically it is felt as crepitus
In the trauma situation, its presence indicates possible serious injuries that do require urgent management.
RADIOGRAPHY
CHEST X-RAY
There are often striated lucencies in the soft tissues that may outline muscle fibers. It can outline the pectoralis major, giving rise to the ginkgo leaf sign. Often there are displaced rib fractures indicating a cause of the gas.
CT
Subcutaneous emphysema is visible on CT scans, with pockets of gas seen as extremely dark low attenuation areas in the subcutaneous space.
USG
Well defined comet tail artefacts can be seen

MECHANISM OF ACTION:
ADH is secreted in response to:
Volume depletion (ECF) detected by low-pressure baroreceptors in great veins, atria and pulmonary vessels, and high-pressure baroreceptors in the carotid sinus and aortic arch
Angiotensin II (AGII)
EFFECTS:
It regulates Total Body Water (TBW).
The specific renal effects of ADH on water balance include:
OTHER EFFECTS

VASOPRESSIN RECEPTOR AGONISTS
Arginine-Vasopressin: A V receptor agonist is a potent alternative to vasoconstrictors in the treatment of fluid and catecholamine-refractory septic shock
Terlipressin is a selective V1 receptor agonist and may be more potent than arginine-vasopressin in restoring catecholamine refractory septic shock
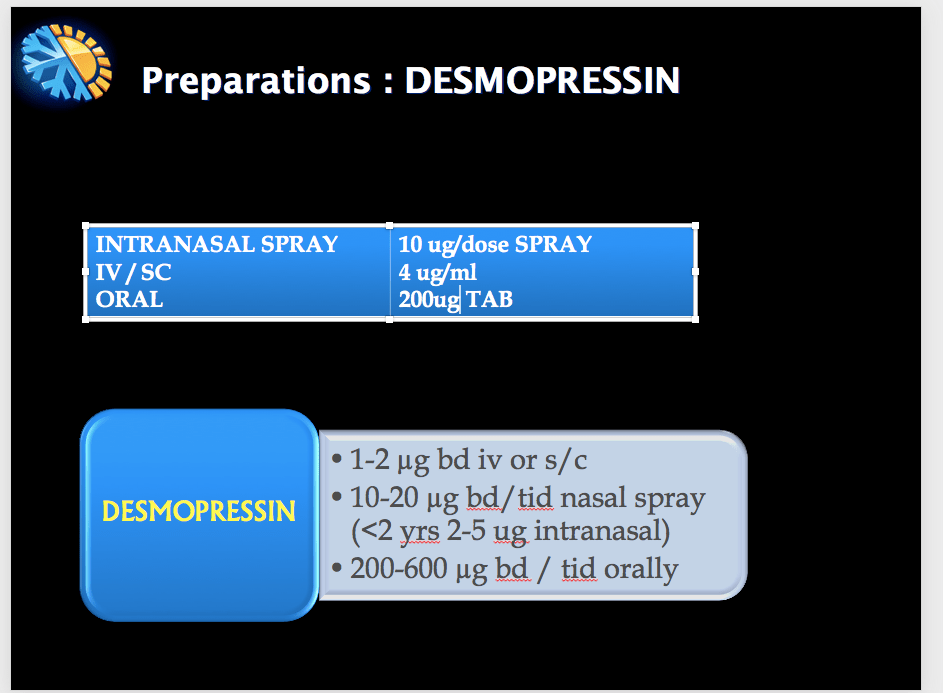
Desmopressin (1-deamino-8-D-arginine vasopressin) is a synthetic vasopressin analog, that acts as an agonist at V1B and V2 receptors. Exhibits antidiuretic and haemostatic properties. So also used in the management of some forms of hemophilia and von Willebrand’s disease

ANTAGONISTS
Vaptans act by inhibiting vasopressin’s action on all the 3 types of receptors. e.g. Conivaptan (unselective), Tolvaptan (V2 selective). Used in the treatment of euvolemic (eg SIADH) and hypervolemic (CHF) hyponatremias, nehrogenic DI, cirrhosis, PCKD etc
Plasma calcium < 2.2 mmol/L
Normal values: Total calcium 2.25-2.60 mmol/L; ionised calcium 1.12-1.32 mmol/L
HYPOCALCAEMIA CAUSES:
Decreased parathyroid hormone
Decreased Vitamin D activity (e.g. intestinal malabsorption, liver disease, CRF)
Increased calcium loss (e.g. chelating agents, calcification of soft tissues)
Decreased ionised calcium (e.g. alkalosis)
CLINICAL FEATURES:
ECG:
QTc prolongation by prolonging the ST segment
Torsades de pointes and atrial fibrillation in severe cases
NB: The corrected QT interval (QTc) is taken as the time between the beginning of the QRS complex and the end of the T wave, it is less than 440 ms in men and 460 ms in women. Severe hypocalcaemia (less than 1.9 mmol/L) may cause a prolongation of the QTc. A QTc greater than 500 ms is associated with an increased risk of Torsades de Pointes.
TREATMENT:
COURSE:
BRANCHES:
The muscular branches:
The cutaneous branches:
The posterior interosseous nerve (terminal branch), passes into the posterior compartment of the forearm. It supplies supinator, many extensors and abductor pollicis longus. It also supplies the wrist joint.
The superficial radial nerve (terminal branch) is entirely sensory. It divides into dorsal digital nerves and supply the dorsal aspect of the hand upto the radial half of the ring finger.
CAUSES OF RADIAL NERVE INJURY:
DEFINITION:
Pain is ‘an unpleasant sensory and emotional experience associated with actual or potential tissue damage’. (IASP: International Association for the Study of Pain)
CLASSIFICATION:
According to chronicity
According to nature
Nociceptive pain: Pain occurring due to stimulation of peripheral sensory nerve fibres (nociceptors) that respond to potentially harmful stimuli; further divided into
Neuropathic pain: Pain that occurs due to a primary lesion or dysfunction in the nervous system itself.
THE GATE CONTROL THEORY OF PAIN:
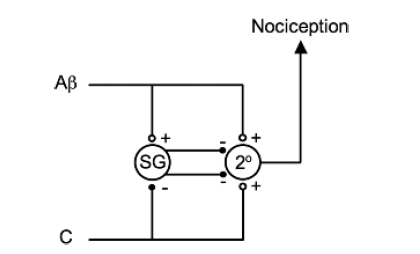
The Aβ fibres are examples of afferents that stimulate inhibitory interneurones (in the substantia gelatinosa (SG)) and, therefore, prevent nociceptive transmission to the CNS. The C fibres are examples of afferents that inhibit inhibitory interneurones and, therefore, enhance nociceptive transmission. Note that both types of fibres stimulate the second-order neurone (2°) directly but it is the interneurone that modifies the transmission.
Laminae 2 & 3 are called the substantia gelatinosa and is the site of the ‘gate control theory’ of pain.
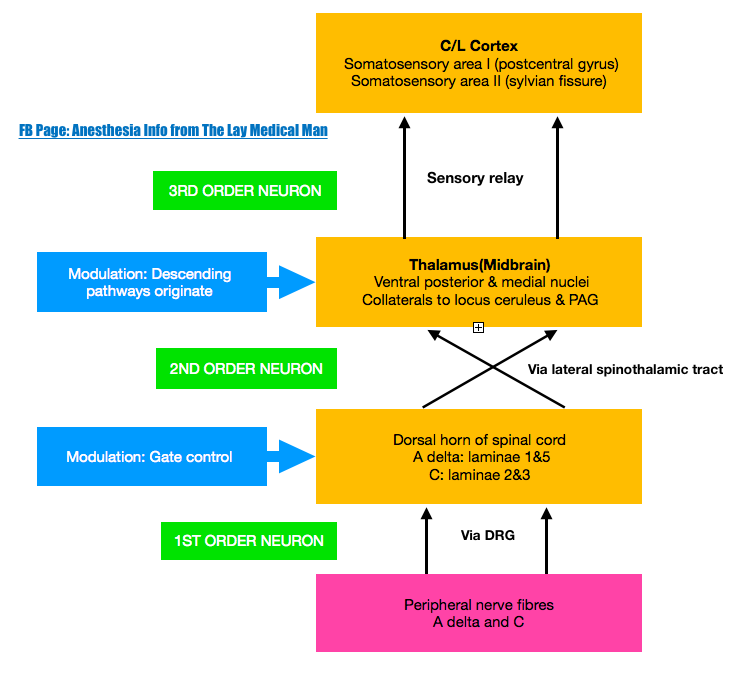
PAIN PATHWAY
There are three levels of neuronal involvement and the signals may be modulated at two points during their course to the cerebral cortex. Descending inhibitory pathways arise in the midbrain and pass to the dorsal horn. Multiple different neurotransmitters are involved in the pathway and include GABA,NMDA, noradrenaline and opioids.
Noxious stimuli –>tissue damage –>mediators–> nociceptors stimulation–> action potential –> propagated along afferent nerve fibres C & Aδ –> dorsal horn of the spinal cord –> Synaptic transmission with secondary interneurones occurs in Rexed’s laminae –> secondary interneurones decussate and travel in the anterolateral spinothalamic tracts –> through the brainstem –>to the thalamus –> tertiary afferents project to the somatosensory cortex.
Some spinal ascending fibres transmit impulses to the reticular-activating system, and to higher centres involved with affect, emotion and memory.
Descending fibres from cortex, thalamus and brainstem exert an inhibitory influence on pain transmission in the dorsal horn
An immediate polysynaptic withdrawal reflex occurs at the level of the spinal cord as some interneurones connect to motor neurones at many levels. This is a protective reflex.
DESCENDING INHIBITORY PATHWAYS
Periaqueductal grey (PAG) in the midbrain receives projections from the thalamus, hypothalamus, amygdala and cortex, and delivers projections to the nucleus raphe magnus (NRM) in the medulla, whose fibres synapse in the substantia gelatinosa of the dorsal horn. Its transmitters include endorphins and enkephalins (MOP opioid receptors) and serotonin (5HT1 and 5HT3 receptors).
Locus caeruleus (LC) is an important brainstem nucleus projecting descending inhibitory pathways to the dorsal horn via noradrenaline (α-adrenergic receptors).
PARACETAMOL:
Central action via COX 3 inhibition which is associated with decreased brain PGE2 levels. It also modulates endogenous cannabinoid system
MORPHINE:
Morphine work by stimulating presynaptic Gi-protein-coupled MOP and KOP opioid receptors. Binding of the ligand causes the following events:
> Closure of voltage-gated Ca2+ channels
> Decreased cAMP production
> Stimulation of K+ efflux from the cell
> Hyperpolarisation of the cell membrane.
> This leads to decreased excitability of the cell and therefore decreased neurotransmitter release and pain transmission
