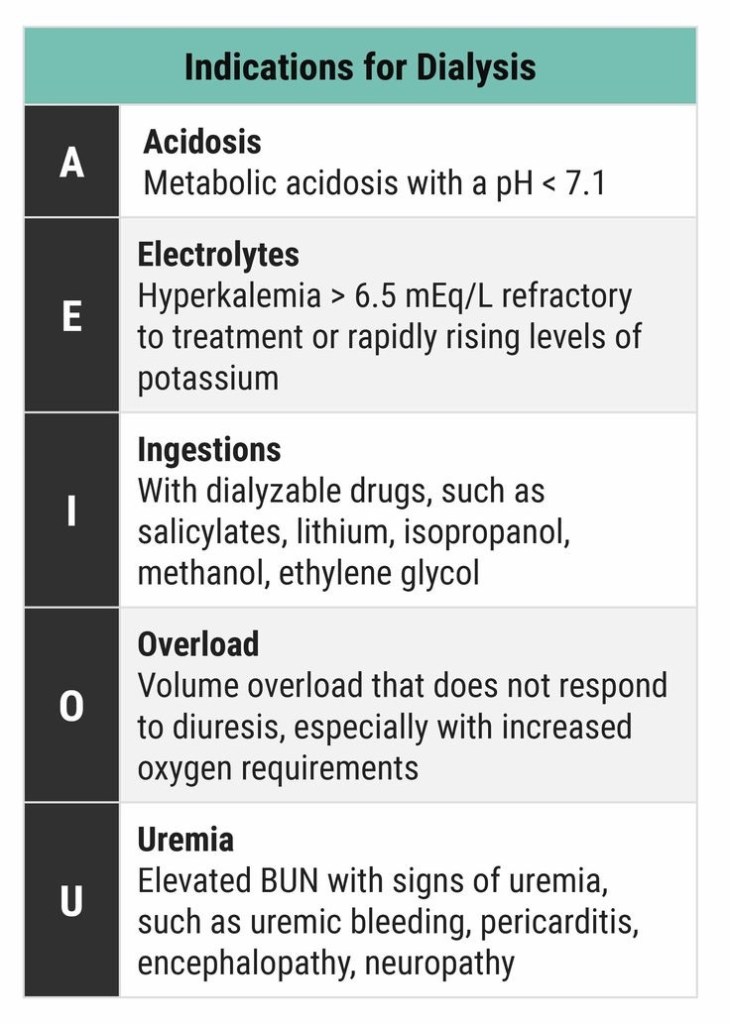
DIALYSIS INDICATIONS
Plasma calcium < 2.2 mmol/L
Normal values: Total calcium 2.25-2.60 mmol/L; ionised calcium 1.12-1.32 mmol/L
HYPOCALCAEMIA CAUSES:
Decreased parathyroid hormone
Decreased Vitamin D activity (e.g. intestinal malabsorption, liver disease, CRF)
Increased calcium loss (e.g. chelating agents, calcification of soft tissues)
Decreased ionised calcium (e.g. alkalosis)
CLINICAL FEATURES:
ECG:
QTc prolongation by prolonging the ST segment
Torsades de pointes and atrial fibrillation in severe cases
NB: The corrected QT interval (QTc) is taken as the time between the beginning of the QRS complex and the end of the T wave, it is less than 440 ms in men and 460 ms in women. Severe hypocalcaemia (less than 1.9 mmol/L) may cause a prolongation of the QTc. A QTc greater than 500 ms is associated with an increased risk of Torsades de Pointes.
TREATMENT: