Category Archives: Critical Care
DELIRIUM IN ICU PPT
COVID TIPS FOR THE ANAESTHETIST

N95 MASK DISINFECTION.

HEY ANESTHESIOLOGIST!
1.TAKE CARE OF YOURSELF
2.ASK OPINION TO SOMEONE WHO ALREADY HAD AN EXPERIENCE
3.GOOD COMMUNICATION BETWEEN ANESTHESIA & SURGERY TEAMS
4.PLAN SUFFICIENTLY EARLY AND DISCUSS INSIDE THE TEAM
5.ASSIGN DUTIES CLEARLY TO EACH MEMBER

COVID 19 AND THE ANAESTHESIOLOGIST: WHAT EXACTLY YOU WILL DO WHEN MANAGING A COVID POSITIVE PATIENT IN OR/ICU OR DURING CPR? A SUMMARY OF 8 SOCIETY GUIDELINES
GENERAL INSTRUCTIONS FOR PERIOPERATIVE SCENARIO (Source: 1 Consensus guidelines for managing the airway in patients with COVID-19 Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists, Source: 2 Editorial, anesthesia-analgesia, May 2020, Source: 3 Anesthesia Patient Safety Foundation and World Federation of Societies of Anesthesiologists, accessed 3/13/2020, Source: 4 Interim guidance for health care providers during covid-19 outbreak from AHA and 5 CDC guidelines)
- Remember that your personal protection is the priority. Plan ahead as it takes time to apply all the barrier precautions. Before intubation, review and practice donning and doffing the appropriate respiratory protection, gloves, face shield, and clothing.
- Practice appropriate hand hygiene before and after all procedures.
- Anaesthesia/ Intubating personnel should don full PPE (Well fitting N95 mask, goggles+ face shield, splash resistant gown, boot covers, double gloves)
- Patient should wear a mask; continue it during pre-oxygenation
- When intubated patient being transferred to ICU or transfer from one circuit / ventilator to other, avoid disconnections in patient’s breathing circuit. Put the ventilator on stand by to turn off flows. Clamp ETT with forceps to prevent aerosolization
- Tracheal intubation of the COVID positive patient is a high risk procedure for the staff, irrespective of the clinical severity of the disease. Do not rush; priority should be to succeed in the first chance. Avoid unreliable, unfamiliar or repeated techniques
- Know and communicate the plan before entering the room (Use a checklist). Also plan how to communicate once inside the Operating Room (OR) (It will be difficult with the PPE; You may have to use adequate volume while speaking). You can display your plan/algorithm in the OR.
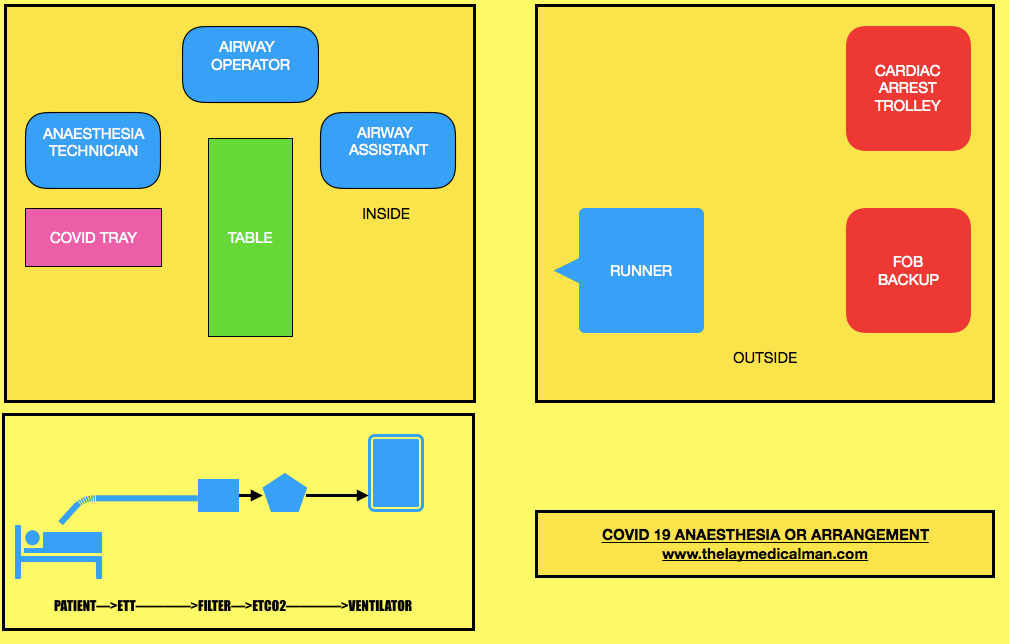
- Limit staff present at the tracheal intubation: one intubator, one assistant and one to give drugs, equipments and monitor the patient; A runner should be there outside the room. The most experienced anaesthetist available should perform the intubation, to maximise first-pass success. Technician/assistant to keep a distance of 2 m from patient
- Touch as less as possible once inside the room
- Ideally we should intubate in a negative pressure room with >12 air changes per hour
- If this is not available, switch off air conditioner/ positive pressure, 20 minutes before and 20 mins after Aerosol Generating Procedures
PREPARATION OF DRUG/ EQUIPMENT
PROCEDURE:

- Most of this should happen outside the room
- Pre-procedure machine check to ensure no leak. Check circuit
- Create a COVID Intubation Trolley (This can also be used in the ICUs)
- Arrange N95 mask and 2 HEPA filters to attach between tracheal tube and breathing circuit and between expiratory limb and anaesthesia machine
- Standard monitors, cannulas, instruments, drugs
- If patient is on HCQ, it will be better to avoid glycopyrrolate and ondansetron
- Sterile plastic covers: for protecting monitors, ventilator or anaesthesia machine and for covering the cable covering the laryngoscope handle. Also keep stylet, appropriate size cuffed tube,10 ml syringe for cuff inflation, oral suction catheter etc
- Face mask
- Airways
- A second generation Supra Glottic Airway device for airway rescue
- Use 5 minutes of preoxygenation with 100% oxygen and RSI techniques to avoid manual ventilation of patient’s lungs and the potential aerosolization of virus from airways.
- No bag mask manual ventilation. Holding the mask: 2-person, 2-handed, with a VE grip technique (rather than the C- technique) to improve seal. If you are forced to mask ventilate, use a 2-person, low flow, low pressure technique
- Intubating dose of Rocuronium or Suxamethonium should be given along with propofol or ketamine (can avoid cardiovascular collapse in some situations): Intubate after 90 seconds (prevent coughing)
- Indirect laryngoscopy with video laryngoscope & intubation under the transparent plastic sheet on the patient
- Inflate the ETT cuff immediately after tube placement, before starting ventilation
- HEPA shield antiviral filter connected to ETT & then connect ETT to ventilator breathing circuit
- Avoid all Aerosol Generating Procedures (AGP) like high flow nasal oxygen, NIV, bronchoscopy and tracheal suction without a closed suction facility. Routine use of supraglottic airway devices unless in unanticipated difficult airway should be avoided
- Use a closed suction system
- Confirm correct position of the tracheal tube. Confirmation of the ETT position will be difficult while wearing PPE; so for this purpose we may have to rely on inspection of bilateral chest examination, observation of ETCO2 waveforms etc.
- Have a vasopressor ready for managing hypotension if it happen post-intubation
- Push-twist all connections to avoid circuit disconnections
- Clamp tube and pause ventilator for all airway manoeuvres and for attempting to resolve circuit disconnections
- Place a nasogastric tube if necessary.
- If COVID-19 status has not been confirmed, take a deep tracheal aspirate using closed suction
- Institute mechanical ventilation and stabilize patient, as appropriate.
- Lung protective ventilation strategies: Small TV:6 ml/Kg [Predicted body wt= Ht in cm-100 (males) & Ht- 110 (females)]. Plateau pressure </= 30 cm H2O. PEEP= 10-15 mm Hg, Adjust FiO2 to achieve reasonable PaO2 (>60 mm Hg). Target SaO2 88-95%. pH >/= 7.25 (Permissive Hypercapnia)
- Use only metered dose inhalers if bronchodilators indicated at any point ( avoid nebulisation)
- Use of intravenous anesthesia would be preferred to the use of a volatile gas anesthetic machine in the ICU environment, especially given that many of these patients are not going to be rapidly recovered and extubated following the procedure. (Source:6)
- Rule out pneumothorax if there is difficulty in ventilation ( Lung USG, CXR)
- Clean the room 20 minutes after tracheal intubation or any AGP.
- Use low gas flows and closed circuits
- Prophylactic anti emetic before extubation
- Adequate Pain management: Morphine/Fentanyl boluses
- All efforts to prevent coughing including lidocaine/dexmedetomidine
- To prevent aerosol generation extubation also should be performed under transparent sheet
- O2 by nasal cannula / face mask. When wearing nasal prongs, a surgical mask can be worn by the patient over the prongs to reduce droplet spread. Should higher oxygen requirements necessitate use of a mask, non-rebreather masks with an attached exhalation filter can be used.
- NIV or High flow O2 can cause aerosol generation: so better to avoid
- Ensure the availability of ambu bag with filter during transfer
- After leaving the room, do a meticulous doffing of PPE
- In the ICU: The use of CPAP/BiPAP may increase the risk of delayed deterioration leading to need for emergent intubation and increased risk of mistakes in donning PPE due to time pressures to resuscitate. In general, CPAP/BiPAP should be avoided in patients with Covid 19 and should never be used outside of appropriate airborne/droplet isolation.
- All airway equipment must be decontaminated and disinfected according to appropriate hospital policies.
- After removing protective equipment, avoid touching hair or face before washing hands.
- NB: N95 mask disinfection: Either cycle through 4 masks in series: one for each day, then repeat (OR heat the mask to 70 degree for 30 minutes (UV light, alcohol, bleach and touching the metal of the oven during heating…all these can degrade the mask)
EMERGENCY INTUBATION IN THE CRITICAL CARE UNIT (Source: 6 Wax, R.S., Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth/J Can Anesth(2020))
- Here also the same principles cited above should apply; additional points are
- Higher level of precautions are needed here as there is high-level viral shedding due to severity of patient illness and procedures associated with resuscitation or intubation may generate aerosols
- All personnel in the room must be using appropriate PPE, including either a fit-tested N95 mask or a PAPR. The procedure should be attempted by the most skilled person. Recurrent traffic of people bringing equipment into the room may increase the risk of viral transmission.
- Clinicians should strongly consider pneumothorax in any ventilated patient with sudden respiratory deterioration. Portable ultrasound may be used to quickly assist in the diagnosis of a pneumothorax, as arranging for a CXR will lead to delay in intervention.
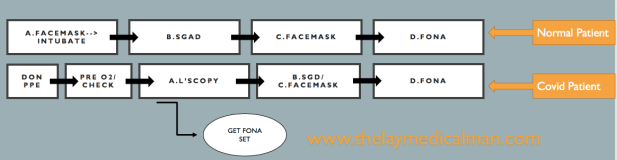
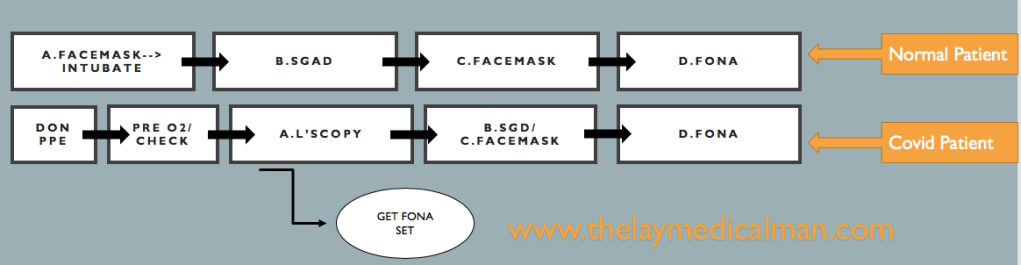
DIFFICULT AIRWAY
Compared to the normal patient, after the first failure of intubation itself, we should order for Front Of Neck Access (FONA) set. And in the next step, we can either do step B (SGD) or step C ( Facemask). Because of this, we will move fast towards the final step of FONA in the Covid difficult airway algorithm.
Prevention and management of respiratory or cardiac arrest: Protected Code Blue (PCB) (Source: 7 Resuscitation Council. Resuscitation Council UK Statement on COVID-19 in relation to CPR and resuscitation in healthcare settings. 2020. Source: 8 Wax, R.S., Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth/J Can Anesth(2020))
- Do not listen or feel for breathing by placing your ear and cheek close to the patient’s mouth
- Full Aerosal Generating Procedure (AGP) Personal Protective Equipment (PPE) must be worn by all members of the resuscitation/emergency team before entering the room.
- Sets of AGP PPE must be readily available where resuscitation equipment is being locally stored.
- No chest compressions or airway procedures such as those detailed below should be undertaken without full AGP PPE.
- Once suitably clothed, start compression-only CPR and monitor the patient’s cardiac arrest rhythm as soon as possible.
- Do not do mouth-to-mouth ventilation or use a pocket mask. If the patient is already receiving supplemental oxygen therapy using a face mask, leave the mask on the patient’s face during chest compressions as this may limit aerosol spread.
- If not in situ, but one is readily available, put a simple oxygen mask on the patient’s face. Restrict the number of staff in the room (if a single room). Allocate a gatekeeper to do this.
- Tracheal intubation or SGA insertion must only be attempted by individuals who are experienced and competent in this procedure.
- Dispose of, or clean, all equipment used during CPR following the manufacturer’s recommendations and local guidelines.
- Any work surfaces used for airway/resuscitation equipment will also need to be cleaned according to local guidelines.
- Specifically, ensure equipment used in airway interventions (e.g. laryngoscopes, face masks) is not left lying on the patient’s pillow, but is instead placed in a tray.
- Do not leave the Yankauer sucker placed under the patient’s pillow; instead, put the contaminated end of the Yankauer inside a disposable glove.
Lower risk resuscitation interventions:
| Placement of an oral airway |
| Placement of an oxygen mask with exhalation filter on patient (if available) |
| Chest compressions |
| Defibrillation, cardioversion, transcutaneous pacing |
| Obtaining intravenous or intraosseous access |
| Administration of intravenous resuscitation drugs |
Higher risk resuscitation interventions more likely to generate aerosol and/or increase risk of viral transmission to staff
| Bag-mask ventilation |
| CPAP/BiPAP |
| Endotracheal intubation/surgical airway |
| Bronchoscopy |
| Gastrointestinal endoscopy |
NEWER ANTIPLATELET, ANTICOAGULANT, FIBRINOLYTIC AND ANTIFIBRINOLYTIC AGENTS
ANTIPLATELET DRUGS
INHIBITORS OF Tx A2 PATHWAY
ASPIRIN: Aspirin inhibits TXA2 synthesis by irreversibly acetylating cyclooxygenase-1
INHIBITORS OF ADP RECEPTOR P2Y12
CLOPIDOGREL: Clopidogrel is a thienopyridine that irreversibly inhibits P2Y12 on the platelet surface. It’s a prodrug and must be metabolized in the liver to generate the active metabolites that inhibit the ADP receptor. The limitations are that it’s anti platelet action has a ceiling effect, and some patients are resistant to the effects of clopidogrel. Should be stopped at least 7 days prior to the surgery.
PRASUGREL: Prasugrel is also a thienopyridine that requires hepatic metabolism to generate active metabolites. But as this metabolism is more efficient than that of clopidogrel, prasugrel produces more rapid, more consistent, and more potent inhibition of ADP-induced platelet aggregation than clopidogrel does. Furthermore, the polymorphisms in CYP2C19 and CYP2C9 that limit the effectiveness of clopidogrel do not affect . Should be stopped at least 7 days prior to the surgery.
CANGRELOR: Cangrelor, which is administered intravenously, has a rapid onset and offset of action.
TICAGRELOR: Ticagrelor is an orally active inhibitor of P2Y12 that provides more rapid and complete antiplatelet effect than clopidogrel. Should be stopped at least 5 days prior to the surgery.
TICLOPIDINE: One potential side effect of ticlopidine therapy is neutropenia. Should be stopped at least 14 days prior to the surgery.
PHOSPHODIESTERASE INHIBITORS:
DIPYRIDAMOLE AND CILOSTAZOL: cAMP serves as an intracellular signal to suppress platelet activation and subsequent aggregation. By inhibiting phosphodiesterase, dipyridamole and cilostazol increase the levels of cyclic adenosine monophosphate. The risk of bleeding with these agents appears to be low.
GPIIb/IIIa ANTAGONISTS
ABCIXIMAB: Synthetic antibody which binds strongly to glycoprotein IIb/IIIa receptors (on platelets) thereby blocking the binding of fibrinogen (to platelets) thereby preventing the cross-linking of platelets which is needed for strengthening of the clot. It has the greatest affinity for GP IIb-IIIa among the GP IIb-IIIa antagonists. The prolonged platelet-bound half-life of abciximab accounts for both its prolonged effect on platelet function after termination of infusion and the gradual return of platelet function thereafter. Because the circulating pool of abciximab is bound to platelets, the effects of the agent can be reversed with the transfusion of platelets.
EPTIFIBATIDE AND TIROFIBAN: Both eptifibatide and tirofiban are synthetic antagonists of GP IIb/IIIa receptor.
GP IIb-IIIa antagonists are likely to be of greatest value when short term intense antiplatelet therapy is indicated, such as during PCI
ANTICOAGULANT DRUGS
THROMBIN INHIBITORS
DABIGATRAN ETEXILATE: Dabigatran etexilate, a prodrug, is an oral, direct thrombin inhibitor. Bioavailability is 6%. It can be administered as twice daily dosing. The drug is dialyzable. The effect can be monitored with ecarin clotting time or thrombin time. Dabigatran should be stopped 24-48 hours prior to any surgery. Idarucizumab, a monoclonal antibody, can reverses effects of dabigatran.
ARGATROBAN
It is intravenously administered reversible and a direct thrombin inhibitor approved for the management of acute HIT (type II). Advantages or uniqueness over other thrombin inhibitors includes its elimination through the liver (indication in compromising renal dysfunction) and short elimination half-life (35–40 min) that reveals normalization of aPTT in 2–4 h following discontinuation. However, dose reduction should be considered in critically ill patients and those with heart failure or impaired hepatic dysfunction.
HIRUDINS: LEPIRUDIN AND BIVALIRUDIN
These recombinant hirudins are first-generation direct thrombin inhibitors. They are administered by parenteral route, can accumulate in renal insufficiency and should be monitored using aPTT and ecarin clotting time (ECT).
DIRECT FACTOR Xa INHIBITORS
RIVAROXABAN AND APIXABAN : Are oral factor Xa inhibitors used in VTE prophylaxis. Effect can be monitored with anti Xa activity assay. Prothrombin Complex Concentrate may be used to reverse the effect. They should be stopped 48-72 hours prior to any surgery. An interval of 3 days should be kept before regional anesthesia.
IDRABIOTAPARINUX: is an indirect inhibitor of factor Xa that catalyzes the formation of irreversible antithrombin–factor Xa complexes. Idrabiotaparinux is thus the only one of the new oral or long-acting parenteral anticoagulants to have a specific antidote i.e. Avidin.
FONDAPARINUX: Is administered parenterally. It selectively inhibits factor Xa. It is licensed for use in thromboprophylaxis in medical patients and in patients undergoing major lower limb orthopedic surgery or abdominal surgery. After prophylactic dose at least 36-42 hours should elapse before performing central neuraxial blockade, whereas with therapeutic doses, one should avoid central neuraxial block.In patients with Heparin-induced thrombocytopenia (HIT), fondaparinux is the preferred agent. Prothrombin Complex Concentrate may be used to reverse the effect.
DANAPAROID
Danaparoid is an indirect factor Xa inhibitor with coagulation effects through antithrombin-mediated inhibition of factor Xa. It is a glycosaminoglycan mixture containing 84% heparin sulfate, dermatan sulfate, and chondroitin sulfate resulting in 10% incidence of HIT. It has a long elimination half-life of 22 h that could be prolonged with renal insufficiency. There is no antidote, coagulation monitoring can be done by measuring anti-Xa activity. It cannot be hemofiltered, but can be removed using plasmapheresis. It is used as an alternative in patients with HIT.
LMWH
e.g.: ENOXAPARIN, DALTEPARIN, TINZAPARIN
LMWH has an average molecular weight of 2000–10,000 daltons with a greater ability to inhibit factor Xa, than thrombin. It has a more predictable dose response curve and is administered at fixed dose, based on total body weight. LMWH has 100% bioavailability and reaches peak levels 2–4 h after S/C administration. It has a half-life of 3–4 h, and is eliminated primarily via renal clearance, necessitating dose reduction in patients with renal insufficiency. Factor Xa levels are used to monitor the effects of LMWH; ideally, factor Xa levels should be obtained 4 h after the administration of LMWH. Properties of LMWH differ from UFH in the following ways:
- Lack of monitoring of anticoagulant response (anti-Xa level not predictive of risk)
- Prolonged elimination half-life
- Anti-Xa activity present 12 h postinjection
- Unpredictable response to protamine
THROMBOLYTICS/FIBRINOLYTICS
ALTEPLASE, TENECTEPLASE, UROKINASE
Thrombolytic agents act by converting plasminogen to the natural fibrinolytic agent plasmin. Plasmin lyses the clots by breaking down fibrinogen and fibrin contained in the clot. Clot lysis elevates fibrin split/degradation products. Thrombolytic therapy will maximally depress fibrinogen and plasminogen for 5 h following therapy and remain depressed for 27 h.[25]
Initiation of thrombolytic therapy is contraindicated within 2 day following neuraxial/deep-PNB procedures and surgery; should perform assessments every 2 h for neurological deficits. The 2 day minimum is based on prolonged plasminogen depression for 27 h.
ANTIFIBRINOLYTICS
TRANEXAMIC ACID(TA) AND E-AMINOCAPROIC ACID: Tranexamic acid and ε-aminocaproic acid are synthetic antifibrinolytic amino acids (lysine analogues) that competitively block the lysine-binding site of both plasminogen and plasmin, therefore inhibiting each enzyme action.Plasmin can no longer bind to fibrin and can no longer degrade fibrin, and thus bleeding is reduced. Tranexamic acid and ε-aminocaproic acid have a small molecular weight and half life of about two to three hours. On a molar basis, TA is at least seven times more potent than EACA.
Clinically, tranexamic acid has been shown to increase the risk of seizures in patients undergoing cardiac surgery, largely when moderate and high doses (more than 10mg/kg) are used. Possible causal mechanisms include inhibition of GABA-A and glycine inhibitory receptors leading to stimulation of excitatory pathways, as well as an increased susceptibility of cardiac patients to postoperative seizures due to emboli introduced during surgery.
DOSE TA : 1g or 10mg/kg IV pre-incision bolus; maintenance: 1g iv over 8 hours (trauma) 1-5 mg/kg/hour (cardiac, ortho surgeries)
APROTININ: Aprotinin (a non-specific serine protease inhibitor) inhibits plasmin in a high dose and is the only agent shown to reduce the need for re-exploration.15 However, marketing of the drug was suspended in November 2007 after preliminary results of the BART trial, which showed an increasing mortality trend relative to the lysine analogues.
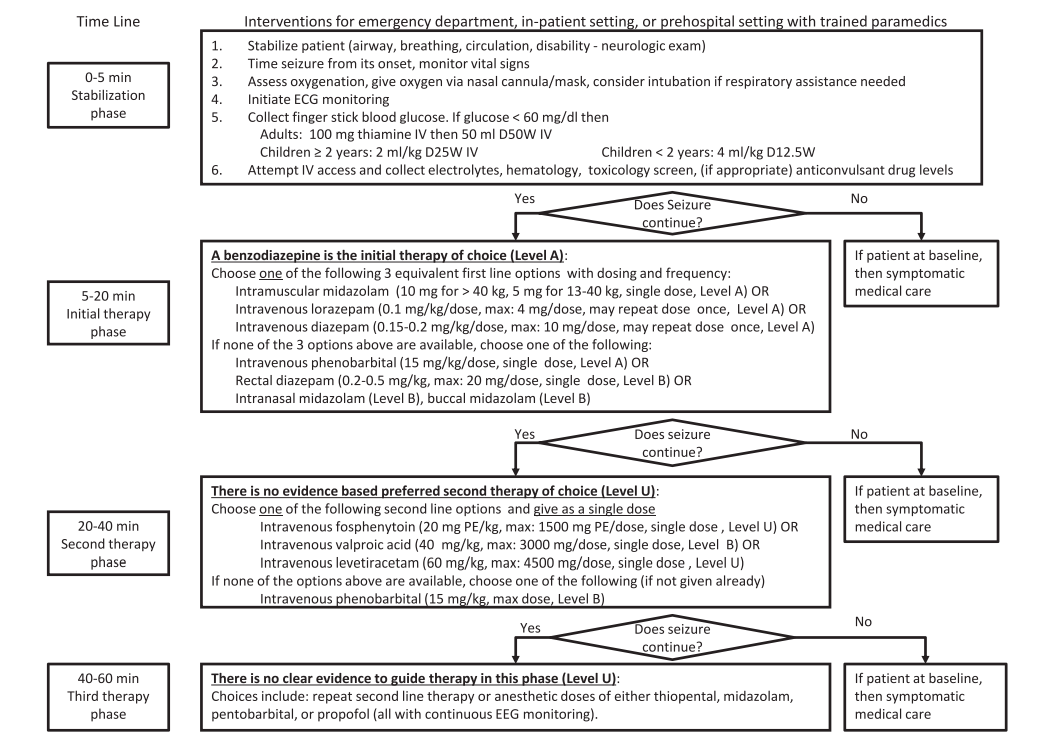
AMERICAN EPILEPSY SOCIETY GUIDELINES 2016: STATUS EPILEPTICUS
VIVA SCENE: NON INVASIVE VENTILATION (NIV)
- NIV is a technique of providing ventilation without the use of an artificial airway.
- NIV has two primary pressure settings
-
The inspiratory positive airway pressure (IPAP) is similar to the peak airway pressure in traditional mechanical ventilation. A higher IPAP level would result in a larger tidal volume and minute ventilation.
-
The expiratory positive airway pressure (EPAP) is the same as PEEP during mechanical ventilation or CPAP during spontaneous breathing. In addition to its ability to improve oxygenation by increasing the functional residual capacity, EPAP also relieves upper airway obstruction with its splinting action.
-
SpO2, Capnography, PaO2, PaCO2 etc may be used for the titration of appropriate IPAP and EPAP levels.
-
CPAP (Continuous positive airway pressure) provides positive airway pressure during spontaneous breaths and it does not include any mechanical breaths. For this reason, the work of breathing is entirely assumed by the patient. CPAP is active when IPAP=EPAP. CPAP is the treatment of choice for obstructive sleep apnea without significant carbon dioxide retention. CPAP should not be used in apnea due to neuromuscular causes, if there is progressive hypoventilation or facial trauma
-
Bilevel PAP (Bilevel positive airway pressure) provides IPAP which controls peak inspiratory pressure during inspiration and EPAP that controls end-expiratory pressure. Indications are acute respiratory failure and acute hypercapnic exacerbations of COPD
-
In patients with acute cardiogenic pulmonary edema, CPAP or bilevel PAP ventilation has been found to reduce the need for subsequent mechanical ventilation
-
Inability to protect the airway from secretions or aspiration, apnoea, facial trauma are contraindications for NPPV.
- We can use nasal or oronasal mask as the interface for delivering NIV
VIVA SCENE: SUBCUTANEOUS EMPHYSEMA – RADIOLOGY
Subcutaneous emphysema, refers to gas in the subcutaneous tissues
Clinically it is felt as crepitus
In the trauma situation, its presence indicates possible serious injuries that do require urgent management.
RADIOGRAPHY
CHEST X-RAY
There are often striated lucencies in the soft tissues that may outline muscle fibers. It can outline the pectoralis major, giving rise to the ginkgo leaf sign. Often there are displaced rib fractures indicating a cause of the gas.
CT
Subcutaneous emphysema is visible on CT scans, with pockets of gas seen as extremely dark low attenuation areas in the subcutaneous space.
USG
Well defined comet tail artefacts can be seen
