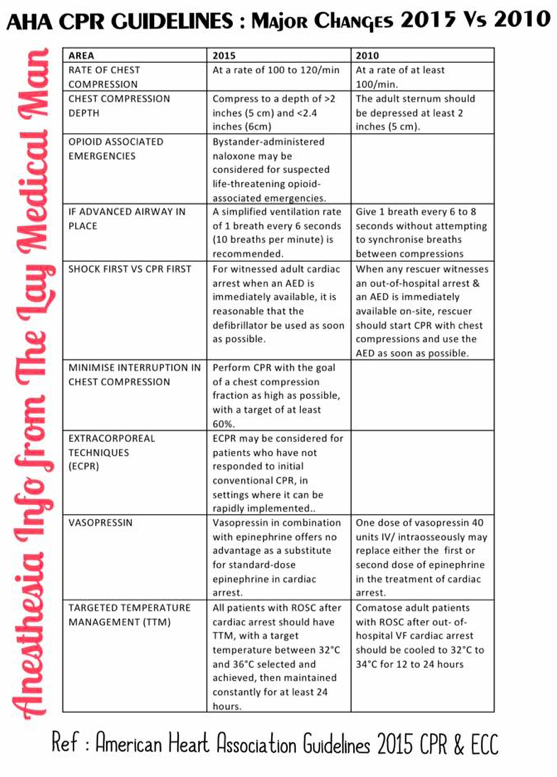
Sorry. Please note that the DATA IN THE FIRST TWO COLUMNS HAVE TO BE INTERCHANGED. i.e. Regarding the RATE and DEPTH of compression, “at least” specification has come in the 2015 GUIDELINES
Sorry. Please note that the DATA IN THE FIRST TWO COLUMNS HAVE TO BE INTERCHANGED. i.e. Regarding the RATE and DEPTH of compression, “at least” specification has come in the 2015 GUIDELINES
What’s the problem, if we place the temperature probe in upper 1/3rd or 2/3rd of the esophagus?
Esophageal temperature should be taken from the lower third of the oesophagus; placed above this level, the probe may under-read due to cooling effect of inspired gases. It gives a good estimate of cerebral blood temperature.
What’s the advantage of nasopharyngeal temperature measurement over oesophageal measurement?
The nasopharyngeal temperature probe is placed just behind the soft palate. The advantage is that it is more accessible compared to the oesophageal temperature measurement. The disadvantage is that it is less accurate in representating the core temperature.
What are the advantages of measurement of temperature @ Tympanic membrane?
The tympanic membrane provides an accurate representation of hypothalamic temperature. It is less invasive, has a short response time and correlates well with oesophageal temperature. But it does not allow continuous measurements.
What is the best method for CONTINUOUS measurement of core temperature?
Blood temperature measurement using a pulmonary artery flotation catheter
What are the factors reducing the accuracy of Rectal temperature measurement?
Rectal temperature is influenced by heat generated from gut flora, the cooling effect of blood returning from the lower limbs and the insulation of the probe by faeces. It is normally about 0.5–1.0 ° C higher than core temperature and has a slow response time.
Can you say an e.g. of utilising the temperature gradients existing between different sites of the body for clinical advantage?
The gradient between a skin temperature and a core temperature can be used as a marker of peripheral perfusion.
Train of four (TOF)
four stimuli {T1-T4} are given at a frequency of 2 Hz (0.5 sec between the stimuli)
Each stimulus in the train causes the muscle to contract and the ‘fade’ in the response allow us to evaluate the neuro muscular blockade
The ratio T4:T1 ( i.e. Dividing the amplitude of the fourth response by the amplitude of the first response ) indicates the degree of neuromuscular block.
Non-depolarizing NMBAs produce a decrease in magnitude of the first twitch compared with a pre-relaxant stimulus, and a progressive reduction in magnitude of T1–T4.
The number of elicited twitches indicates the degree of receptor occupancy.
Disappearance of T4, T3, T2, T1 corresponds to 75%, 80%, 90% and 100% occupancy.
With recovery of neuromuscular function the twitches appear in the reverse order.
Accepted values for TOF count are:
1 twitch for tracheal intubation
1–2 twitches during established anaesthesia
3–4 twitches before reversal of neuromuscular blockade is attempted.
Double burst stimulation
Consists of two bursts ( the duration of each square wave impulse in the burst is 0.2 sec ) at 50 Hz with each triple burst separated by 750 ms.
DBS with 3 impulses in each of the two tetanic bursts is commonly used
These manifest visually as two separate stimuli (T1 and T2).
The ratio is related to the TOF ratio and is easier for the operator to interpret reliably.
Used under light paralysis where train of four ratio is difficult to distinguish
Post-tetanic Count (PTC)
PTC is used when there is no response to TOF stimuli and also when we want to eliminate sudden movements of the patient completely as during ophthalmic and neurosurgery
Uses tetanic stimulation at 50 Hz for 5 s to mobilize presynaptic ACh (to ‘kick start’ the nerve under deep paralysis) .
After a recovery time of 3 sec , it’s followed by 20 pulses at 1-2 Hz twitch stimulation
The number of twitches generated (i.e. the post-tetanic count) reflects the degree of neuromuscular blockade.
Shows fade response earlier than train of four
Used under deep paralysis to estimate time to recovery
#nmb ,#anesthesia ,#anaesthesia , #CriticalCare , #NerveStimulator , #AnesthesiaTechnician ,#NurseAnesthetist ,#AnesthesiaEquipment,#Biomedical ,#BiomedicalEquipment
Reference: frca.uk Anesthesia Monitoring Techniques , Miller’s Anesthesia , 7/e
Supplementary oxygen to all hypoxaemic patients with acute severe asthma to maintain an SpO2 level of 94-98%
Nebulisers for giving nebulised β2 agonist bronchodilators should preferably be driven by oxygen. A flow rate of 6 l/min is required to drive most nebulisers
High-dose inhaled β2 agonists as first line agents in patients with acute asthma. Repeat doses of β2 agonists at 15–30 minute intervals or give continuous nebulisation of salbutamol at 5–10 mg/hour (requires appropriate nebuliser) if there is an inadequate response to initial treatment. Higher bolus doses, for example 10 mg of salbutamol, are unlikely to be more effective (2.5–5 mg salbutamol in children >2 years).
There is no evidence for any difference in efficacy between salbutamol and terbutaline. Nebulised adrenaline (epinephrine), a non-selective β2 agonist, does not have significant benefit over salbutamol or terbutaline.
Add nebulised ipratropium bromide (0.5 mg 4-6 hourly) to β2 agonist treatment for patients with acute severe or life-threatening asthma or those with a poor initial response to β2 agonist therapy. ( 250 micrograms/dose in children >2 years).
Consider giving a single dose of IV magnesium sulphate (1.2-2 g IV infusion over 20 minutes) to patients with acute severe asthma who have not had a good initial response to inhaled bronchodilator therapy.
Nebulised magnesium is not recommended for treatment in adults with acute asthma. Consider adding 150 mg magnesium sulphate to each nebulised salbutamol and ipratropium in the first hour in children >2 years with a short duration of acute severe asthma symptoms presenting with an oxygen saturation less than 92%.
Routine prescription of antibiotics is not indicated for patients with acute asthma.
SECOND LINE TREATMENT OF ACUTE ASTHMA
Consider early addition of a single bolus dose of intravenous salbutamol (15 micrograms/kg over 10 minutes) in a severe asthma attack where the patient has not responded to initial inhaled therapy.
Consider aminophylline for children >2 years with severe or life-threatening asthma unresponsive to maximal doses of bronchodilators and steroids. A 5 mg/kg loading dose should be given over 20 minutes with ECG monitoring (omit in those receiving maintenance oral theophyllines) followed by a continuous infusion at 1 mg/kg/hour. Measure serum theophylline levels in patients already receiving oral treatment and in those receiving prolonged treatment.
NOTE:
Give steroids in adequate doses in all cases of acute asthma attack.
Prednisolone 40–50 mg daily or parenteral hydrocortisone 400 mg daily (100 mg six-hourly in adults and 4 mg/kg repeated four hourly in children >2 years ) are as effective as higher doses. Continue prednisolone 40–50 mg daily for at least five days or until recovery. ( In children >2 years, treatment for up to three days is usually sufficient).
Following recovery from the acute asthma attack steroids can be stopped abruptly. Doses do not need tapering provided the patient receives Inhaled Corticosteroids
In adults with an acute asthma attack, i.v. aminophylline is not likely to result in any additional bronchodilation compared to standard care with inhaled bronchodilators and steroids. Side effects such as arrhythmias and vomiting are increased if Iv aminophylline is used
Heliox is not recommended for use in patients with acute asthma outside a clinical trial setting
Although theoretically furosemide may produce bronchodilation, a review of three small trials failed to show any significant benefit of treatment with nebulised furosemide compared to β 2 agonists
NICE published guidelines in 2006, revised in 2011.
Step 1 : Choose either an ACE inhibitor, a thiazide diuretic or a calcium channel antagonist (A, D and C).
An ACE inhibitor is more effective as first-line therapy in younger patients (< 55 years ) and Caucasians.
Diuretics or calcium channel blockers are better in older patients and African / Caribbean patients of any age.
This trial of step 1 is run on for 4 weeks, and if blood pressure is not controlled, the opposite agent is added in:
Step 2 : An ACE inhibitor is added to a diuretic (A + D) or calcium channel antagonist (A + C), or vice versa.
Step 3 : Ongoing poor control is then managed by the addition of the third agent (A + C + D).
Step 4 : If a patient is established on triple therapy, and still not well controlled, they are probably aldosterone sensitive, so spironalactone would be a wise option.
National Institute for Health and Clinical Excellence. Hypertension: Clinical Management of Primary Hypertension in Adults. NICE Clinical Guideline 127, August 2011.
Entonox is Nitrous oxide mixed 50:50 with oxygen
It provides analgesia with maintenance of consciousness.
Usually administered via a demand valve for self administration.
Takes 30 seconds to act and continues for approx. 60 sec after inhalation has stopped
For optimum effect inhalation should start when the contraction tightens. This will co-ordinate the maximal effect with the central painful part of the contraction.
20% N20 is equivalent to 15 mg of subcutaneous morphine.
The optimal analgesic concentration was found to be 70% but some mothers lost consciousness at this concentration
50% N20 in oxygen is safer and this has become standard now
Entonox is the BOC trade name for this gas mixture.
Poynting effect
The Poynting effect involves the dissolution of gaseous O2 when bubbled through liquid N2O, with vaporisation of the liquid to form a gaseous O2/N2O mixture.
Critical & Pseudocritical temperature
The critical temperature of a gas is the maximum temperature at which compression can cause liquefaction. Or it is the temperature above which a substance cannot be liquefied however much pressure is applied. Mixing gases may change their critical temperature.
The pseudocritical temperature applies to a mixture of gases, such as Entonox, and is the temperature at which gas mixtures separate into their component parts.
The Poynting effect produces a 50:50 mixture which reduces the crtical temperature of N20 so Entonox has a pseudocritical temperature of -6 degree.
Entonox
Highest -5.5°C @117 bar
Cylinder -7°C @137 bar
Pipeline -30°C @4 bar
In cylinders it is supplied at a pressure of 137 bar and must be stored above its pseudocritical temperature of -6°C.
Below this temperature the N2O liquefies in a process called lamination. If this occurs a high concentration of O2 will be delivered first with little analgesic effect, but as the cylinder empties the mixture will become progressively more potent and hypoxic as it approaches 100% N2O.
If a cylinder has been exposed to cold below -6 degree C it should be warmed for 5 minutes in a 37 degree C water bath or for 2 hours in a room at 15 degree C. It should then be inverted three times before use.
When delivered via a pipeline at 4.1 bar the pseudocritical temperature is less than -30°C.
Altitude per se has no effect on Entonox.
Reference: www.frca.uk
The placenta forms a barrier to the transfer of drugs between the mother and the fetus, but increasing lipid-solubility, decreasing maternal protein binding, decreasing molecular weight, increased materno-fetal concentration gradient and placental blood flow etc will increase the placental transfer of drugs
The relative distribution of the drug across the placenta is represented by Feto-Maternal (F/M) concentration ratio
Pethidine and diamorphine are both metabolised in the fetus to less lipid-soluble products like norpethidine and morphine respectively, which remain on the fetal side of the placenta. The elimination half-lives of these drugs are also longer in the fetus because of immature hepatic metabolism. This again prolongs its existence in the fetal side.
Lipid solubility of drugs like thiopentone sodium are high; so they cross the placenta easily, and can accumulate as the pH is lower in the fetus
Diazepam is metabolised to less lipid-soluble products. So it can have an F/ M ratio of 2 even one hour after maternal administration.
Local anaesthetic agents are weak bases which are largely UN-IONISED at physiological pH, and cross the placenta readily. Foetal ‘trapping’ occurs only in severe acidosis, when the molecules become IONIZED in the fetal side.
Dynamic or absolute viscosity is a measure of the resistance of a fluid or gas to flow. It is measured using a viscometer or rheometer.
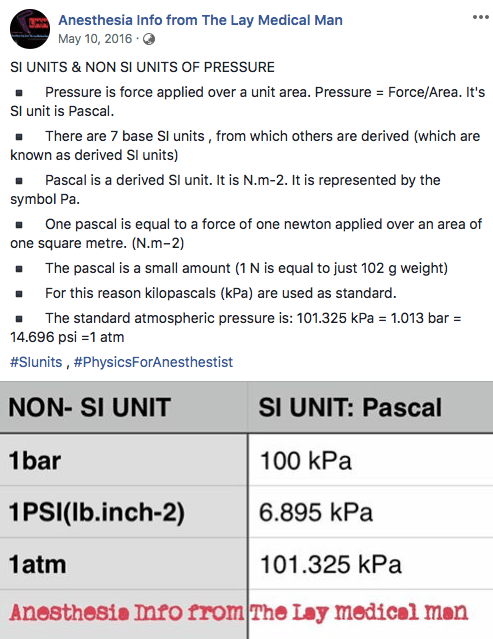
The SI unit of dynamic (or absolute) viscosity is the pascal-second (Pa·s), equivalent to N·s/ m2.
Viscosity is independent of flow rate
Viscosity is independent of pressure
For a gas, viscosity decreases as its temperature increases
The relationship between viscosity and temperature and pressure only holds true for those fluids and gases that exhibit ‘Newtonian’ properties, i.e. substances that will always flow irrespective of forces acting upon them (e.g. crystalloid solutions and water).
Blood is a non-Newtonian fluid and its viscosity depends largely on haematocrit (and varies with flow rate).
Blood viscosity is increased by volatile anaesthetic agents, smoking and aging
A thixotropic substance is one that becomes less viscous over time when agitated. If it becomes more viscous with agitation, this is known as a rheopectic material.
Kinematic velocity is defined as the dynamic velocity of a substance divided by its density.
