# Makes the RBC membrane friable and leads to episodic hemolytic anemia n jaundice
# Stress (surgery or anesthesia), drugs, newborn period, infection, exposure to fava beans are stimulants/risk factors.
# Culprit drug list is long: vit C n K, Methylene blue (caution in rx of methemoglobinemia),SNP, prilocaine.…
# Check for anemia, need for transfusion, jaundice(can also appear postop),cataract(increased incidence)
# Malignant Hyperthermia has been reported in association
# Avoid elective surgeries during a hemolytic episode
# Give a folic acid suppliment perioperatively
# Paracetamol,Phenytoin,L Dopa etc are safe.
Category Archives: Comorbid illness and anesthesia
SJOGRENS SYNDROME-anesthesia implications
![]() 🏳️🌈Preoperative abnormalities
🏳️🌈Preoperative abnormalities
1. Symptoms of the sicca syndrome include dryness of the eyes and skin.
2. Check for associated RA, SLE, scleroderma, the polymyositis, polyarteritis nodosa, chronic active hepatitis, and Grave’s disease.
3.Lung / airway : desiccation of the nose and bronchial tree, obstructive airways disease, interstitial lung disease
4.sensory / motor neuropathy may occur and CNS lesions have been described.
5.The patient may be taking corticosteroids or occasionally immunosuppressive agents.
![]() 🏳️🌈Anaesthetist’s concerns
🏳️🌈Anaesthetist’s concerns
1. Sometimes gross swelling of the salivary glands may make mask anaesthesia difficult.
2.The problems of pulmonary disease, if present.
3.The dry eyes are susceptible to damage during anaesthesia.
4.Allergy to antimicrobial agents, particularly penicillin, cephalosporins and trimethoprim
Management
1. careful assessment of the primary disease, and of any pulmonary involvement.
2. Drying agents should be avoided if possible.
3. The eyes should be protected with pads.
4. Anaesthetic gases should be humidified.
5. Steroid supplements may be required.
6. Care should be taken when prescribing antimicrobial agents
ANESTHESIA IMPLICATIONS-HAEMOCHROMATOSIS
/MNEMO/: ‘HEME LDH’
1. Liver Dysfunction
2. Diabetes
3. Heart Failure
EDTA induced pseudothrombocytopenia:
Problems: unnecessary investigations, delay in doing sx
Steps if suspected (asymptomatic persistent low plt counts):
Rpt PLT COUNT and PERI SMEAR using ANOTHER anticoagulant like heparin/citrate. Or use non-anticoagulated blood taken directly into the platelet counting diluent fluid.. Can see plt clumps in peripheral smear.
HYPOTHYROIDISM: ANESTHESIA CONCERNS
1.Hypothyroidism
2.Anemia
3.Reduced plasma volume
4.Impaired hepatic drug metabolism
5.Hypoglycemia
6.Impaired clearance of free water
7.Hyponatremia
8.Enlarged tongue
9.Nerve compression due to myxoedema
10.Delayed gastric emptying
ANTI #RHEUMATOID AGENTS PERIOPERATIVELY🎲
![]() 🏵 METHOTREXATE: caution in elderly,respiratory-renal-hepatic dysfunction. CONSIDER STOPPING 1 WEEK BEFORE
🏵 METHOTREXATE: caution in elderly,respiratory-renal-hepatic dysfunction. CONSIDER STOPPING 1 WEEK BEFORE
![]() 🏵 SULFASALAZINE: withhold atleast on day of surgery; as elimination is primarily renal and as reduction GFR is possible perioperatively
🏵 SULFASALAZINE: withhold atleast on day of surgery; as elimination is primarily renal and as reduction GFR is possible perioperatively
![]() 🏵 AZATHIOPRINE: withhold on day of surgery
🏵 AZATHIOPRINE: withhold on day of surgery
![]() 🏵 HYDROXYCHLOROQUINE : can continue perioperatively
🏵 HYDROXYCHLOROQUINE : can continue perioperatively
![]() 🏵 LEFLUNOMIDE : decreased wound healing; but stopping <2months prior to surgery unlikely to be beneficial
🏵 LEFLUNOMIDE : decreased wound healing; but stopping <2months prior to surgery unlikely to be beneficial
WHAT YOU WILL SEE IN THE SEROLOGY OF HEPATITIS B INFECTION
1) in a patient recovered from acute HBV: Anti HBsAg , Anti HBcAg Ig G
2) in a C/C carrier : HBsAg , Anti HBcAg Ig G
3) after immunisation : Anti HBsAg
4) best indicator of infectivity: HBeAg
5) best indicator of replication : HBV DNA
6) marker for window period : Anti HBcAg IgM
7) protective antibody : Anti HBsAg
8) acute infection : HBsAg, Anti HBcAg Ig M (plus in high virus load HBeAg and in low level infection Anti HBeAg)
Anesthesia Implications in ACHALASIA CARDIA
MNEMO> First 4 letters of ACHAsia.
A. Acute upper airway obstruction secondary to tracheal compression (by the dilated segment ) can be managed by Sublingual glyceryl nitrate,Passage of a naso-oesophageal tube,Transcutaneous needle puncture,Tracheal intubation etc
C Care against aspiration: The dilated oesophagus must be emptied and decompressed (needs a period of prolonged starvation) Rapid sequence induction ,Tracheal tube removal is performed in the awake patient, Patient should be nursed in the lateral position during recovery.
H History: Respiratory complications, which may be attributed to asthma or chronic bronchitis, are secondary to overspill of undigested material
A Acute problems that can be caused by the dilated segment : Acute thoracic inlet obstruction , difficulty in passing the tracheal tube past the dilated oesophagus, Upper airway obstruction , progressive dilatation of the upper oesophagus may occur in association with air swallowing or IPPV
CARDIAC GRID FOR CONGENITAL HEART DISEASES
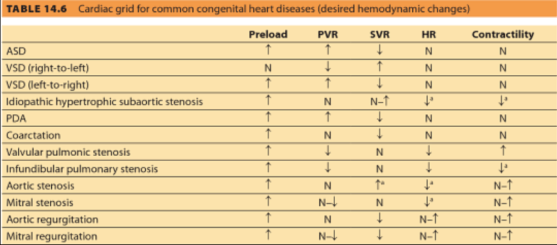
NB:
MITRAL VALVE-AREA
Normal valve surface area 4 – 6 cm2
Symptom free until 1.5 – 2.5 cm2
Moderate stenosis 1 – 1.5 cm2
Critical stenosis <1 cm2
MNEMO🤓 (anaesthesia implications)>Systemic Lupus Erythematosus
” SLE – CARD”
1.Cardiac and Renal involvement![]() 🔻
🔻
2.Anemia![]() 🔻
🔻
3.Raynaud’s phenomenon: So avoid hypothermia![]() 🔻
🔻
4.Determine clotting status![]() 🔻
🔻
![]() 🤓Hint Question: “Have you brought your SLE CARD for surgery?”
🤓Hint Question: “Have you brought your SLE CARD for surgery?”
