1.Hypothyroidism
2.Anemia
3.Reduced plasma volume
4.Impaired hepatic drug metabolism
5.Hypoglycemia
6.Impaired clearance of free water
7.Hyponatremia
8.Enlarged tongue
9.Nerve compression due to myxoedema
10.Delayed gastric emptying
Category Archives: Anesthesia
ANKLE BLOCK : NEEDLE DIRECTIONS
Posterior tibial nerve :
Introduce the needle along the medial aspect of the Achilles tendon, at the level of the cephalic (towards head) border of the medial malleolus. Advance, in an anterior direction, towards the posterior border of the tibia (nerve lies just posterior to the posterior tibial artery).If paraesthesia is felt, inject 3-5ml LA. If not, advance to contact the tibia, withdraw 0.5cm and then inject 5-7ml LA.
Sural nerve :
Introduce the needle along the lateral border of the Achilles tendon at the level of the cephalic border of the lateral malleolus.Advance anteriorly towards the fibula.If parasthesia is felt inject 3-5ml LA. If not, inject 5-7ml LA as the needle is withdrawn. This gives subcutaneous infiltration from the Achilles tendon to the fibula.
Infiltration around the remaining three nerves can be performed from a single site. The needle is inserted 1cm lateral to the tendon of extensor hallucis longis (or just lateral to the anterior tibial artery, if palpable), at the level of the cephalic borders of the malleoli. This tendon is prominent on the dorsum of the foot, during extension of the big toe.
Deep peroneal nerve :
From the position described above, advance the needle posteriorly (i.e. at 90¡ to the skin). Inject 3-5ml LA deep to the fascia, on either side of the anterior tibial artery.
Superficial peroneal nerve :
After blocking the deep peroneal nerve, withdraw the needle to just stay in the skin.
Turn the needle towards the lateral malleolus and inject 5ml LA in a subcutaneous band between the lateral malleolus and the anterior border of the tibia. This should reach all the branches of this nerve.
Saphenous nerve :
Again withdraw the needle to just stay in the skin and turn the needle to point towards the medial malleolus.Infiltrate 5ml LA subcutaneously as the needle is advanced towards the medial malleolus. The great saphenous vein lies in this area, just antero-medial to the medial malleolus, in order to infiltrate around the vein, without causing damage, it may be necessary to make a further skin puncture lateral to the vein.
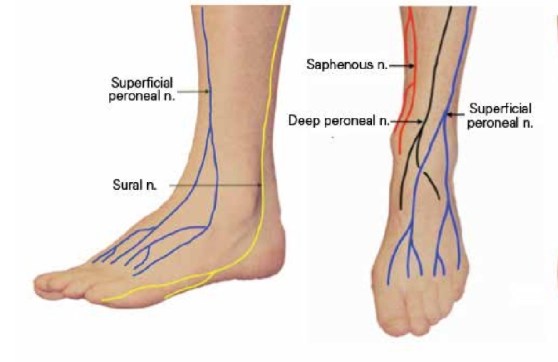
Image courtesy: Semantic Scholar
ANTI #RHEUMATOID AGENTS PERIOPERATIVELY🎲
![]() 🏵 METHOTREXATE: caution in elderly,respiratory-renal-hepatic dysfunction. CONSIDER STOPPING 1 WEEK BEFORE
🏵 METHOTREXATE: caution in elderly,respiratory-renal-hepatic dysfunction. CONSIDER STOPPING 1 WEEK BEFORE
![]() 🏵 SULFASALAZINE: withhold atleast on day of surgery; as elimination is primarily renal and as reduction GFR is possible perioperatively
🏵 SULFASALAZINE: withhold atleast on day of surgery; as elimination is primarily renal and as reduction GFR is possible perioperatively
![]() 🏵 AZATHIOPRINE: withhold on day of surgery
🏵 AZATHIOPRINE: withhold on day of surgery
![]() 🏵 HYDROXYCHLOROQUINE : can continue perioperatively
🏵 HYDROXYCHLOROQUINE : can continue perioperatively
![]() 🏵 LEFLUNOMIDE : decreased wound healing; but stopping <2months prior to surgery unlikely to be beneficial
🏵 LEFLUNOMIDE : decreased wound healing; but stopping <2months prior to surgery unlikely to be beneficial
Amiodarone
AMIODARONE for arrhythmias
LD 150 mg over 10 mins.
INFUSION: 1mg/min x 6 hrs f/b 0.5mg/ min x 18 hrs
i.e. Load 900 mg in 50 cc syringe pump & give 3.33 ml/hr x 6 hrs f/b 1.66 ml/hr x 18 hrs
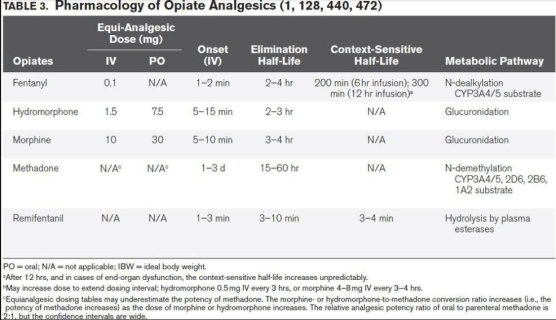
OPIOID PHARMACOLOGY
WHAT YOU WILL SEE IN THE SEROLOGY OF HEPATITIS B INFECTION
1) in a patient recovered from acute HBV: Anti HBsAg , Anti HBcAg Ig G
2) in a C/C carrier : HBsAg , Anti HBcAg Ig G
3) after immunisation : Anti HBsAg
4) best indicator of infectivity: HBeAg
5) best indicator of replication : HBV DNA
6) marker for window period : Anti HBcAg IgM
7) protective antibody : Anti HBsAg
8) acute infection : HBsAg, Anti HBcAg Ig M (plus in high virus load HBeAg and in low level infection Anti HBeAg)
DOSES: TRANSFUSION OF COMPONENTS
![]() 💦 FFP : 15 ml/kg
💦 FFP : 15 ml/kg
![]() 💦 PC :10 ml/kg
💦 PC :10 ml/kg
![]() 💦 F VIII : % of desired rise x body weight x 0.5
💦 F VIII : % of desired rise x body weight x 0.5
Train(ing) of Four
TOF response %of receptors occupied
0 —————–100
1 ——————95
2—————— 90
3 ——————85
4 —————-<75
VIVA AID: IDEAL POSITION OF TIP OF RIGHT IJV CATHETER
- Different methods have been suggested in the literature
- Catheter tips positioned approximately 3 cm below the right tracheobronchial angle will lie in close proximity to the atriocaval junction but will remain extracardiac in location
- Pere P.W. studied correlation between the length of catheter inserted and patient’s height and observed that catheters inserted through right IJV from midcervical point or lower puncture to Height/10cm ended in SVC, while those inserted more than Height/10 + 1cm, 47% ended in right atrium
- Some studies argued that the catheter tip should lie above the pericardial reflection to prevent serious and potentially lethal complications like cardiac tamponade, malignant arrhythmias, placement in coronary sinus and tricuspid valve damage. The upper limit of the pericardial reflection cannot be seen on a plain chest X-ray, but it is generally accepted to be below the carina.
- Most clinicians aim to place the catheter tip at the level of the carina with whichever formula they follow. This position carries the risk of migration, thrombosis, and malfunction.
- A recent paper has demonstrated that a catheter with its tip positioned peripheral to the atriocaval junction was more likely to undergo internal repositioning and venous thrombosis.
- The lower placement is preferred for left-sided IJV cannulations, because aiming the catheter tip placement above the pericardial reflection in this scenario is more likely to lead to oblique placement and abutment against the wall, which is a risk factor for perforation. It seems, therefore, that a free-floating catheter tip in a wider portion of the IJV is more important than placing the catheter above the pericardial reflection.
- This becomes even more relevant in the light of the observations by Schuster and colleagues13 that the pericardium can ascend alongside the medial wall of the SVC by up to 5 cm (mean 3 cm). Thus, catheter tip placement even 3 cm above the SVC–RA junction might not obviate the risk of tamponade in all patients.
- Recently many studies have questioned the placement of the catheter tip in the middle SVC. They argue , emphasizing the importance of having a free-floating tip (not abutting the vessel wall) rather than its placement above the pericardial reflection. This can be achieved by placing the catheter tip in lower SVC and upper RA (target zone, within 2 cm above and 1 cm below the SVC–RA junction). In this position, the SVC is wider, meaning that the catheter tip is likely to float freely with minimal chance of abutment. Furthermore, a catheter placed in this position is amenable to confirmation by TOE.
- Ahn and colleagues have suggested a radiological landmark-based technique for ‘parking’ the catheter within the target zone. They adjudged the depth of CVC insertion by summing [1] the distance between the sternoclavicular joint and the carina (measured offline from the chest radiograph using an internal measuring tool available on the picture archiving and communication system), [2] the distance between the point of insertion and the sternoclavicular joint, and [3] 1.5 cm. The eventual location of the CVC tip was confirmed by TOE. The authors concluded that the catheter tip was positioned more accurately and the determined depth of CVC insertion correlated better with the actual distance from the skin insertion point to the RA–SVC junction with the radiological landmark-based technique compared with Peres’ formula of central venous catheterization via the right IJV
- N.B: Also note that from the right internal jugular and left subclavian approaches, the veins respectively take straight and gently curving trajectories to the superior vena cava. However, the right subclavian vein takes a near-right angle turn into the superior vena cava, and the left internal jugular approach incorporates two turns, one into the brachiocephalic vein and a second into the superior vena cava. These turns create potential for the venous side walls to be punctured by a dilator failing to negotiate a curve appropriately.
-
Ref: Quest to determine the ideal position of the central venous catheter tip D. K. Tempe1,* and S. Hasija, British Journal of Anaesthesia 118 (2): 148–50 (2017)


PAEDIATRIC CAUDAL / EPIDURAL ANAESTHESIA : DRUG DOSING
ARMITAGE : The dosage prescription scheme of Armitage :
With 0.5 mL/kg, all sacral dermatomes are blocked. •
With 1.0 mL/kg, all sacral and lumbar dermatomes are blocked. •
With 1.25 mL/kg, the upper limit of anesthesia is at least midthoracic.
However, when 1.25 mL/kg is injected there is a danger of excessive rostral spread (above T4); it is therefore preferable not to administer more than 1.0 mL/kg of local anesthetic.
EPIDURAL:
Bupivacaine, levobupivacaine- initial dose : Solution: 0.25% with 5 µg/mL (1/200,000) epinephrine
Dose:<20 kg: 0.75 mL/kg20-40 kg: 8-10 mL (or 0.1 mL/year/number of metameres)>40 kg: same as for adults
Continuous infusion- maximum doses: <4 mo: 0.2 mg/kg/hr (0.15 mL/kg/hr of a 0.125% solution or 0.3 mL/kg/hr of a 0.0625% solution)4-18 mo: 0.25 mg/kg/hr (0.2 mL/kg/hr of a 0.125% solution or 0.4 mL/kg/hr of a 0.0625% solution)>18 mo: 0.3-0.375 mg/kg/hr (0.3 mL/kg/hr of a 0.125% solution or 0.6 mL/kg/hr of a 0.0625% solution
Ropivacaine : initial dose: Ropivacaine : 0.2% Dose: same regimen in mL/kg as for bupivacaine (see above)
Infusion : Same age-related infusion rates in mg/kg/hr as for bupivacaine (usual concentration of ropivacaine: 0.1%, 0.15%, or 0.2%)Do not infuse for more than 36 hr in infants < 3 ms
DOSING ACCORDING TO SEGMENT :
The volume of local anesthetic necessary for analgesia/anesthesia depends on location of surgery and epidural catheter. In young children the estimated volume would be: 0.04 mL/kg/segment. In children older than 10 years of age simple formula can be used: V (in mL) = 1/10 x (age in years).
TEST DOSE: The recommended test dose is 0.1mL/kg of local anesthetic with 5mcg/mL of epinephrine to maximum volume of 3mL (or 2.5 mcg/mL in the child less than 18 month old )
