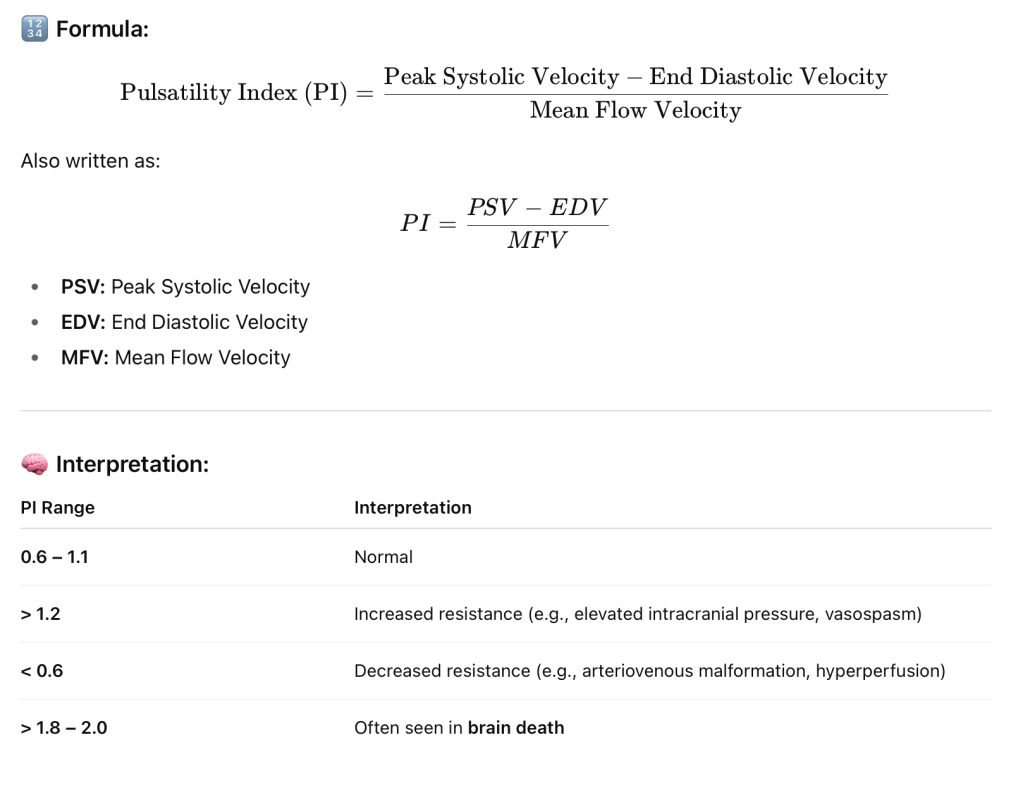
The TCD Pulsatility Index (PI) is a parameter used in Transcranial Doppler (TCD) ultrasonography to evaluate the resistance to blood flow in cerebral vessels. It’s commonly used to assess cerebral hemodynamics, especially in patients with conditions like stroke, traumatic brain injury, hydrocephalus, and brain death.
📌 Clinical Uses of PI in TCD:
Elevated ICP (Intracranial Pressure): Higher PI suggests rising ICP.
Vasospasm detection in subarachnoid hemorrhage.
Brain death evaluation: Very high PI or absent diastolic flow.
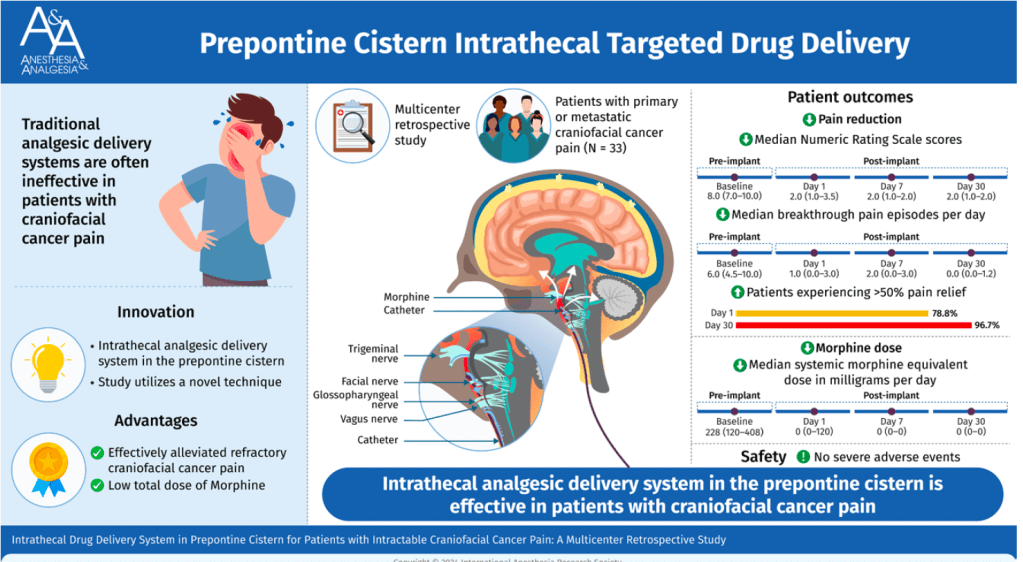
Placing the catheter tip of an intrathecal morphine pump into the prepontine cistern could effectively relieve refractory craniofacial cancer pain with an extremely low total morphine dose requirement and few adverse events. This procedure could be considered in patients with severe refractory craniofacial cancer pain. (Anesth Analg 2025;141:255–63)
Blood transfusion in pediatric neurosurgery, particularly for procedures like craniosynostosis repair, requires a careful and calculated approach. The unique physiological characteristics of children—especially infants—demand precise blood volume estimation, loss assessment, and transfusion decision-making to ensure safety and optimal outcomes.
Below are key calculations and considerations when planning for blood transfusion in pediatric neurosurgical settings:
1. Estimated Blood Volume (EBV)
Understanding the Estimated Blood Volume (EBV) is essential for predicting transfusion needs.
Age Group
Estimated Blood Volume (ml/kg)
Preterm neonates
90–100
Full-term neonates
85–90
Infants (<12 months)
80
Children (>12 months)
75
For example, in craniosynostosis surgeries, which often involve infants, use 80 ml/kg; for children like a 5-year-old patient, use 75 ml/kg.
2. Maximum Allowable Blood Loss (MABL)
To guide intraoperative transfusion decisions, MABL is calculated as:
Massive transfusion (>50% EBV in 3 hrs or 100% in 24 hrs)
Use PRBC : FFP : Platelet = 2 : 1 : 1
Summary
In pediatric neurosurgery, particularly in high-risk procedures like craniosynostosis repair, blood transfusion must be:
✅ Carefully calculated using weight-based formulas ✅ Guided by clinical condition, not just haemoglobin numbers ✅ Continuously reassessed using haematocrit, ABG, and coagulation studies ✅ Supported by a multidisciplinary team for timely intervention
By integrating these evidence-based parameters into your intraoperative workflow, you can significantly improve transfusion safety and patient outcomes.