AEQ 2: Pulmonary Function Tests (PFT)
- Anaesthesia Exam Question 2
- PFTs are done to evaluate the mechanical and gas exchange functions of the lung; most important of these include :
- Spirometry
- Lung Volumes & Elasticity
- Gas Exchange Function Tests
- SPIROMETRY
- It’s the measurement of dynamic lung volumes during forced expiration and inspiration. It includes
- Forced Vital Capacity (FVC)
- Forced Expiratory Volume in one second (FEV1) &
- Maximum expiratory flow during the middle 50% (25-75%) of the vital capacity- this is a sensitive index of small airway obstruction
- The severity of COPD is graded based on the FEV1 values:
- Mild COPD- FEV1 >70% of predicted
- Moderate COPD- FEV1 50-69% of predicted
- Severe COPD- FEV1 <50% of predicted
- In COPD and asthma, the FEV1 will be reduced more markedly than FVC resulting in a reduction in FEV1/FVC ratio (>70%)
- The response to bronchodilators in the form of an increase in FEV1 and FVC indicates reversibility and helps in diagnosis- a response >15% from the baseline value shows significant reversibility and points towards a diagnosis of bronchial asthma
- TLC and RV will be increased in COPD
- THE FLOW VOLUME(FV) LOOPS

- The normal FV loop:
- The patient takes a vital capacity breath and starts the test with a forced expiration
- The loop rises rapidly to a flow rate of 8-10 l/sec followed by a steady decrease as the expiration continue from left to right- the patient will be unable to cross the maximal flow line because of the dynamic compression of the airways. So the normal loop represents the maximum flow rate at each lung volume
- Then inspiration occurs from RV to TLC in a right to left direction to achieve a flow rate of 4-6 l/sec and has a squarer shape

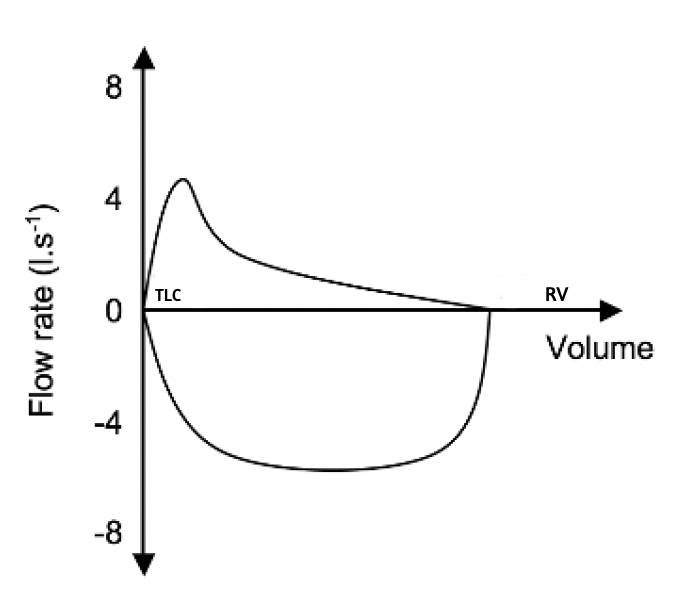
- FV loop: COPD
- COPD reduces flow rates all through the expiration with increased concavity or a ‘scooped out’ appearance of the expiratory limb. PEFR is also reduced
- Due to gas trapping, the RV (and TLC) is increased. The inspiratory flow rates are only slightly reduced
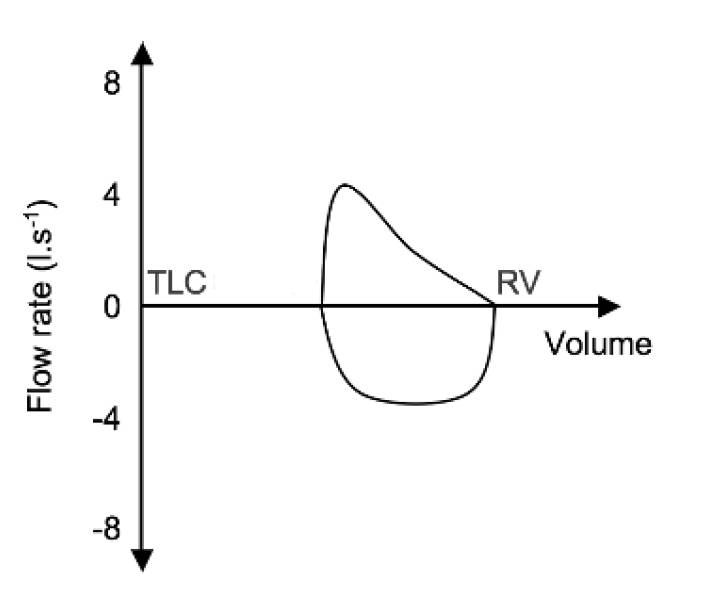
- FV loop: Restrictive Diseases
- Restrictive diseases shifts the left hand side of the curve towards right because of a marked reduction in TLC while preserving RV. PEFR is also reduced.

- FV loop: Variable Extrathoracic Obstruction – Problem: during inspiration
- e.g. Laryngomalacia, vocal cord paralysis, subglottic stenosis, goitres, tracheomalacia of extrathoracic trachea
- The negative pressure generated in the airway during inspiration makes the airway collapse thus markedly reducing the inspiratory flow, but retains the square shape
- The positive pressure generated during expiration, keeps the airway open. So the expiratory limb may be near normal
- The TLC and RV are generally unaffected.
- FV Loop: Variable Intrathoracic Obstruction
- e.g. Tracheomalacia of intrathoracic trachea and tracheal tumours
- If the obstruction is intrathoracic, the negative pressure generated in the intrapleural compartment during inspiration will help to pull and open up the airways. So the inspiratory limb will be near normal.
- The positive pressure generated during expiration will make the airway further narrower. So the expiratory flow will be markedly reduced, similar to that happens in COPD.
- The TLC and RV are generally unaffected.
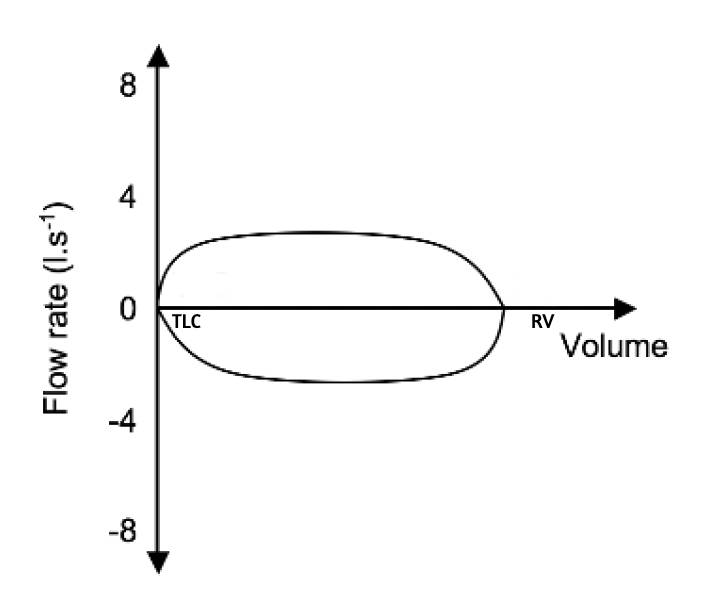
- FV Loop: Fixed Large Airway Obstruction
- e.g. Tracheal stenosis
- Here the peak expiratory and inspiratory flows are determined by the diameter of the orifice- so both the expiratory and inspiratory limbs show markedly reduced flow.
- The TLC and RV are generally unaffected.
- GAS EXCHANGE FUNCTION TESTS
- TLCO measures the integrity and functioning of the gas exchange surface of the lung. This will be reduced in emphysema and is also a good indicator of the severity of the disease. PEFR is also reduced.
- Arterial Blood Gas analysis and Exercise testing are additional tests that will reflect the functioning of lung function
AEQ1: Revised Cardiac Risk Index (RCRI) and ACS-NSQIP
- Anaesthesia Exam Question:1
- Revised Cardiac Risk Index (RCRI) is one of the commonly used perioperative risk indices
- The RCRI determines preoperative risk based on risk of surgery, history of ischemic heart disease, congestive heart failure, cerebrovascular disease, preoperative use of insulin and creatinine greater than 2.0 mg/ dL.
- The total score ranges from 0 to 6, with higher scores indicating a higher risk of major adverse cardiac events (MACE). The risk categories and their corresponding scores are as follows:
- 0 points: Low risk (MACE rate <1%)
- 1-2 points: Intermediate risk (MACE rate 1-5%)
- 3-6 points: High risk (MACE rate >5%)
- RCRI is less accurate in patients undergoing vascular, noncardiac surgery. In addition, as RCRI does not capture risk factors for noncardiac causes of perioperative mortality, it does not predict all-cause mortality well
- American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) is a universal surgical risk calculator model developed using a web-based tool . The ACS-NSQIP calculator incorporates 20 patient risk factors in addition to the surgical procedure. From this input, it calculates the percentage risk of a MACE, death, and 8 other outcomes. This risk calculator may offer the best estimation of surgery-specific risk of a MACE and death. It has excellent performance for predicting mortality and morbidity. It has not been validated in an external population outside the NSQIP. This classification has poor inter-rater reliability
- Surgery-specific risk calculation using ACS-NSQIP report the rate of cardiac death or non-fatal MI and are noted to be greater than 5% in high-risk procedures, 1% to 5% in intermediate-risk procedures, and less than 1% in low-risk procedures. Emergency surgery is associated with higher risk of MACEs compared with elective procedures.
