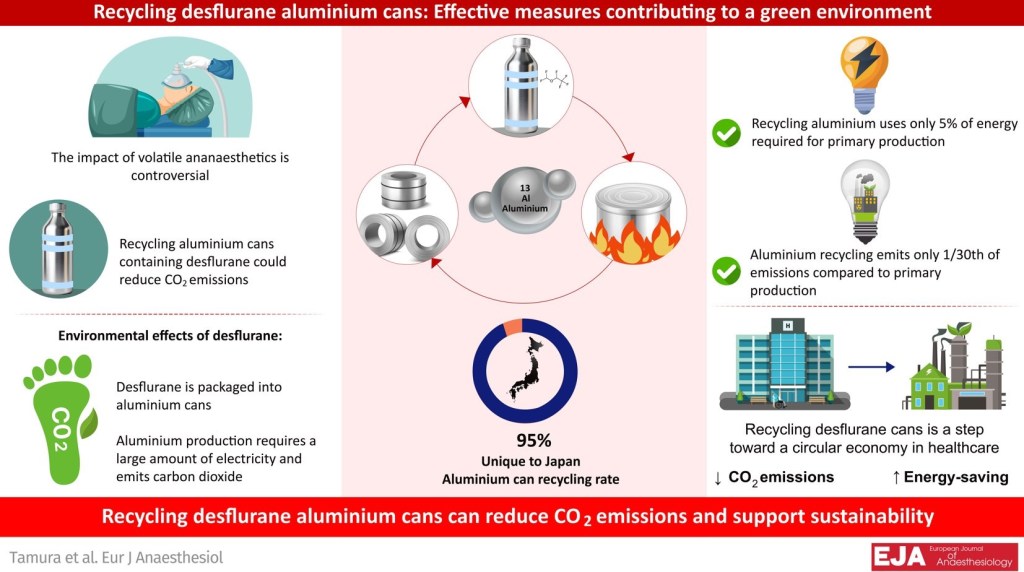
DESFLURANE CANS RECYCLING Posted on June 6, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
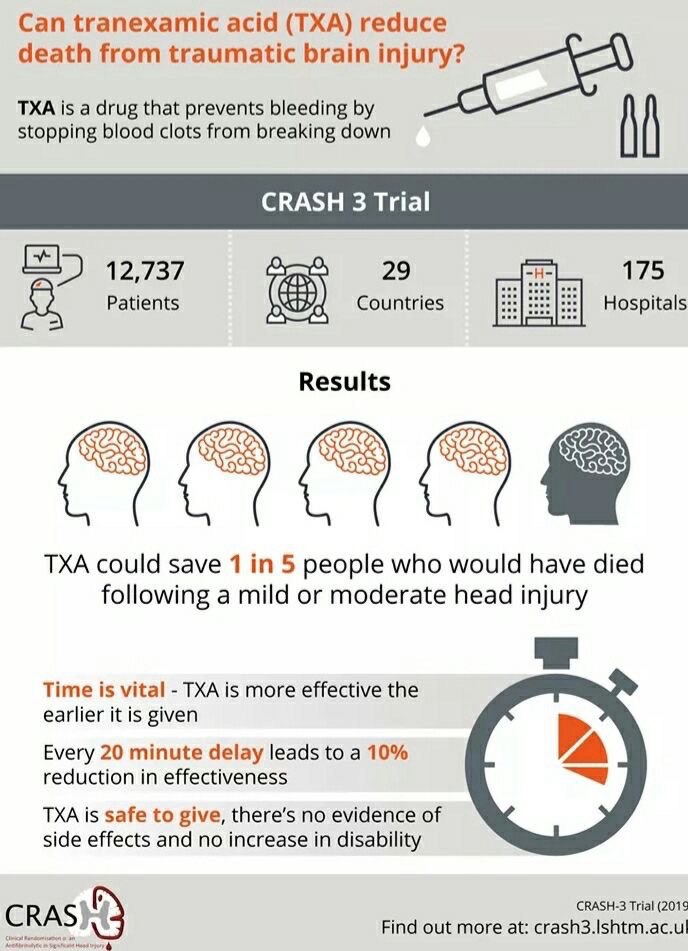
CRASH TRIAL Posted on May 24, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
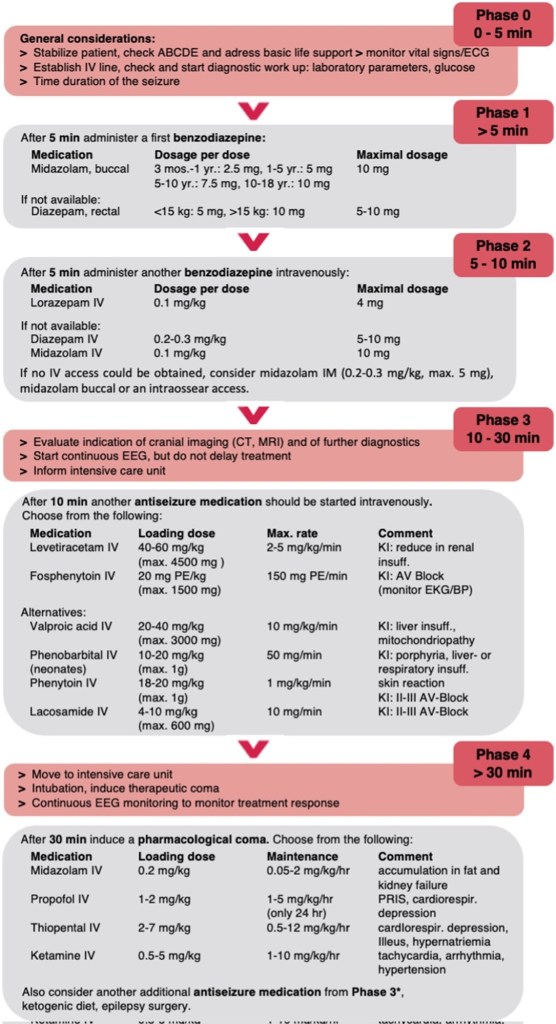
Pediatric Status Epilepticus Management Posted on May 23, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
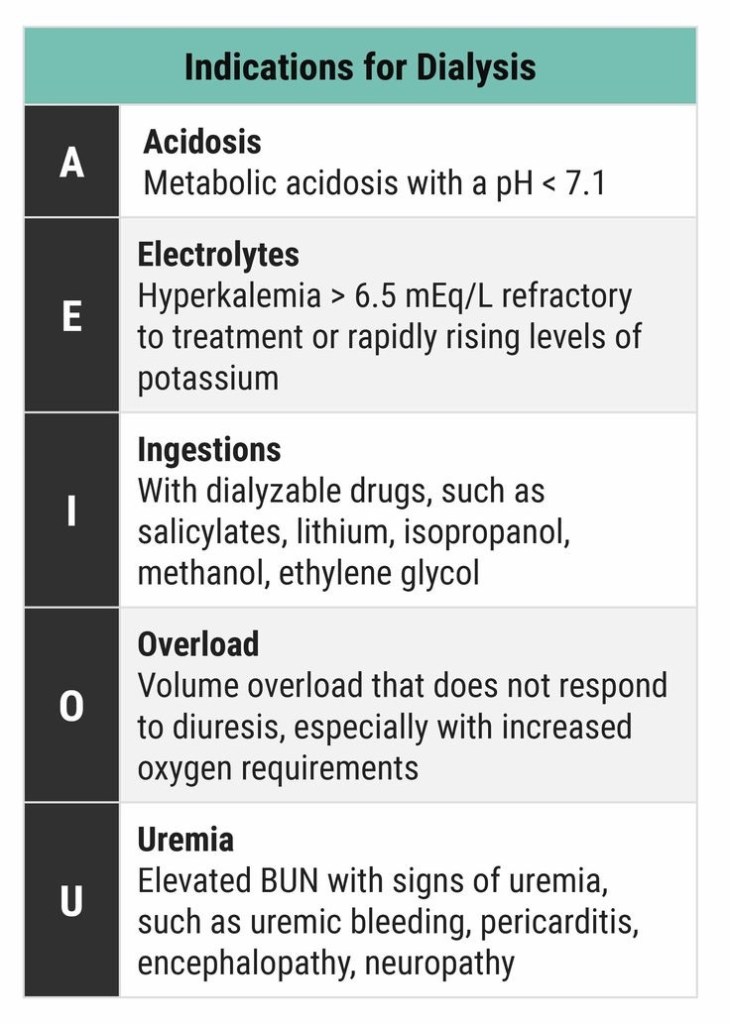
DIALYSIS INDICATIONS Posted on May 20, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
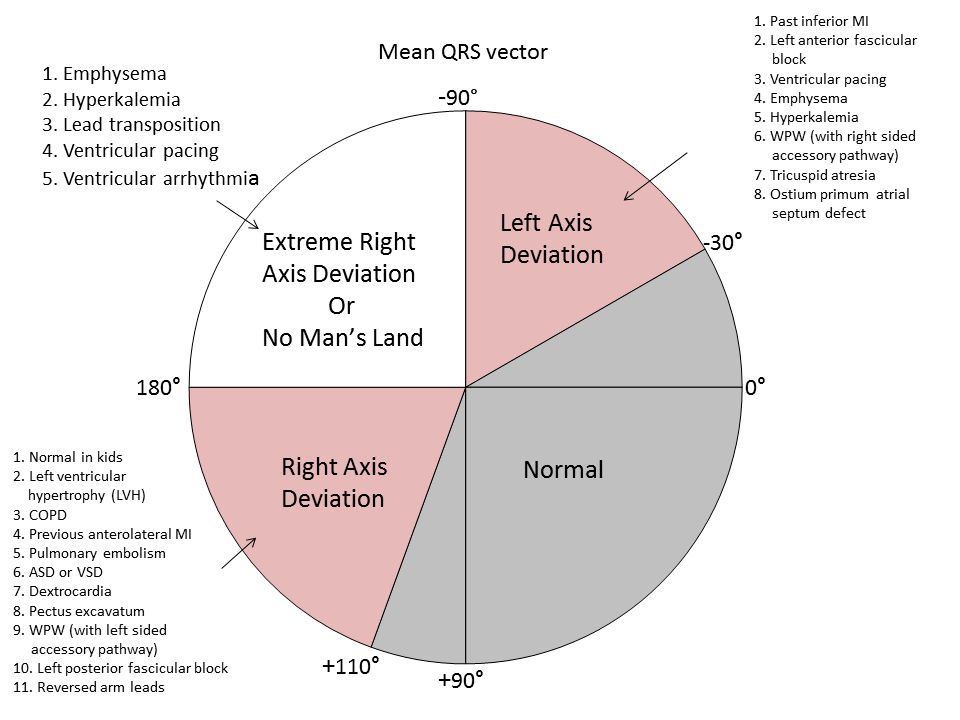
ECG AND AXIS Posted on May 20, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
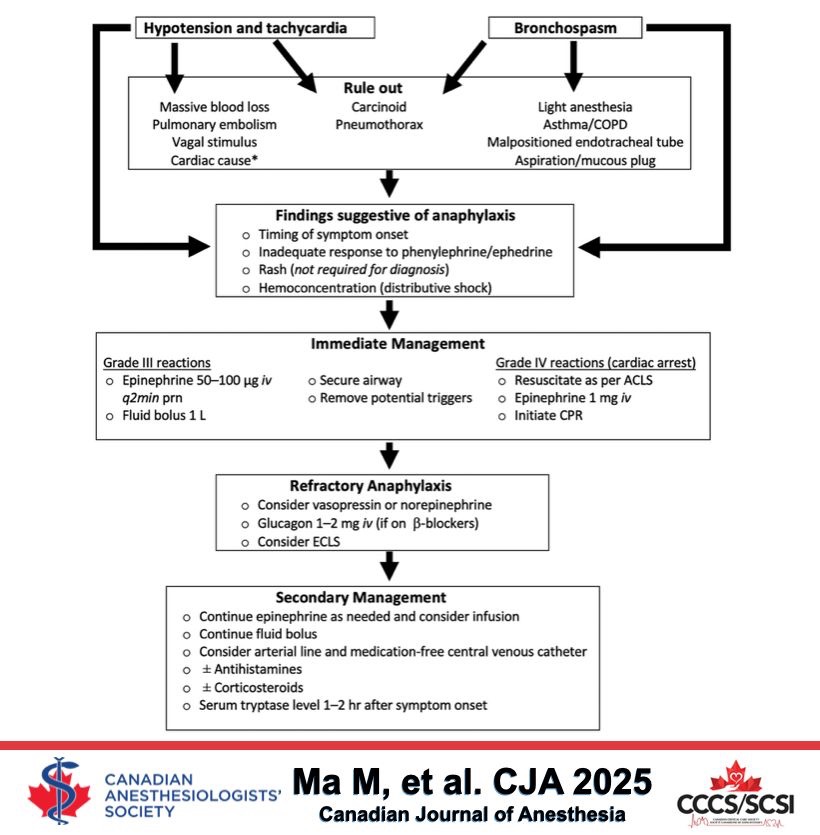
Perioperative Anaphylaxis Posted on May 20, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
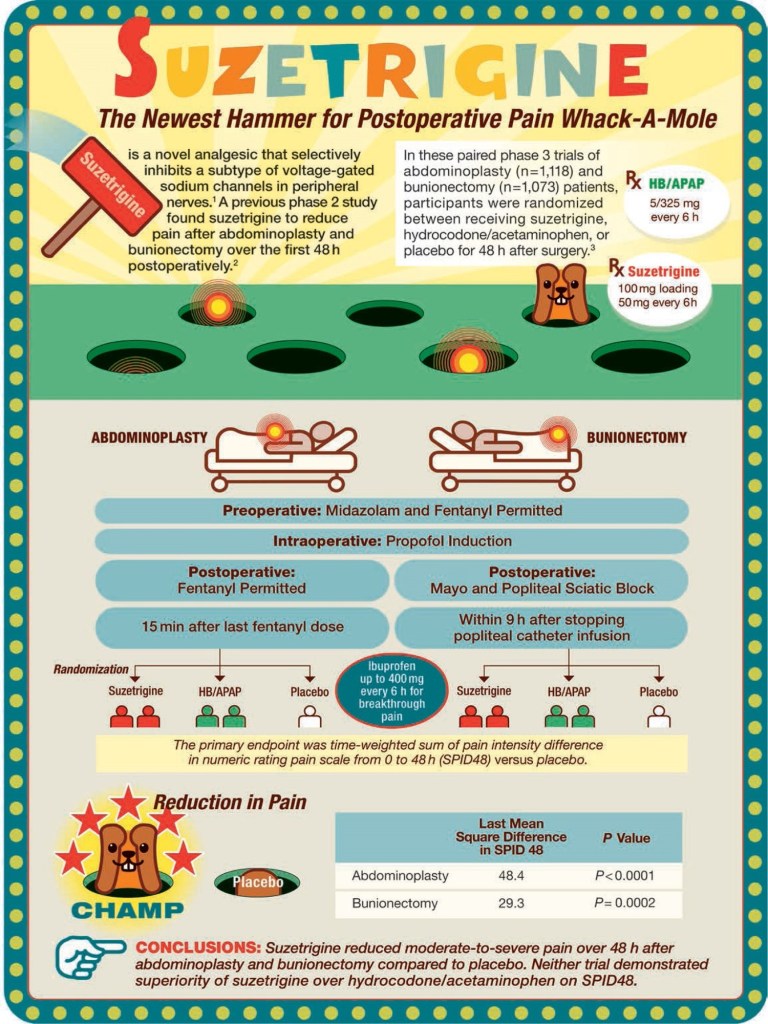
Suzetrigine Posted on May 19, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
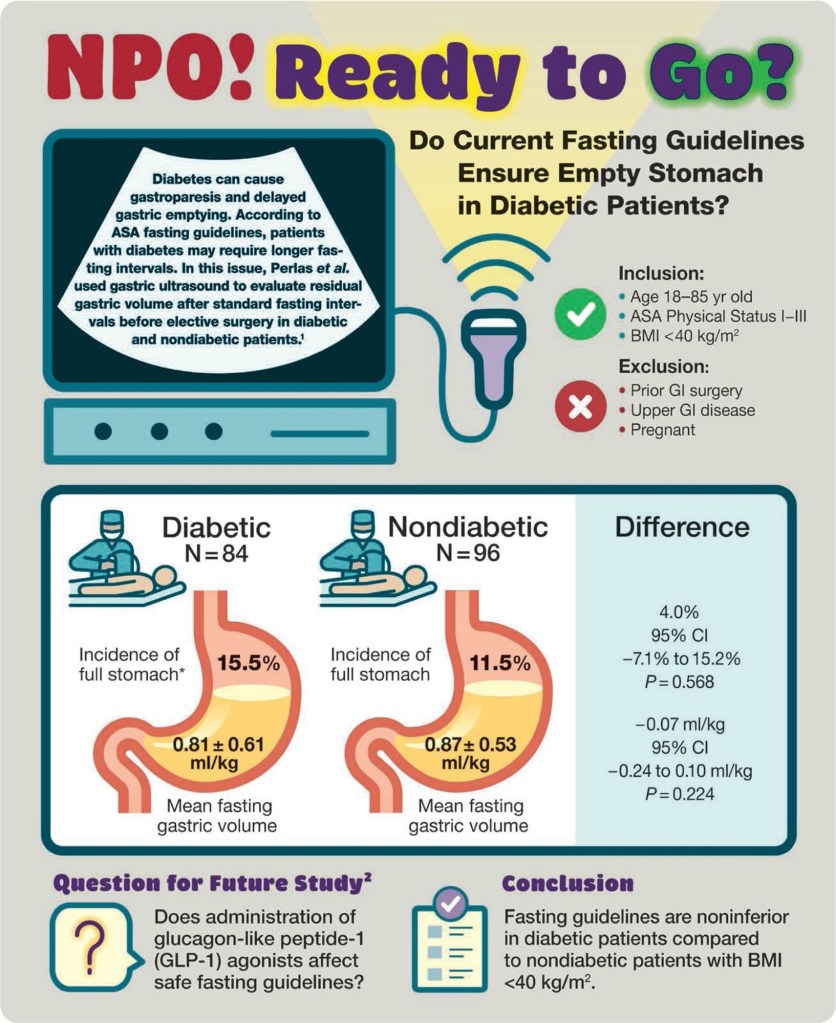
NPO Guidelines in Diabetics Posted on May 6, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
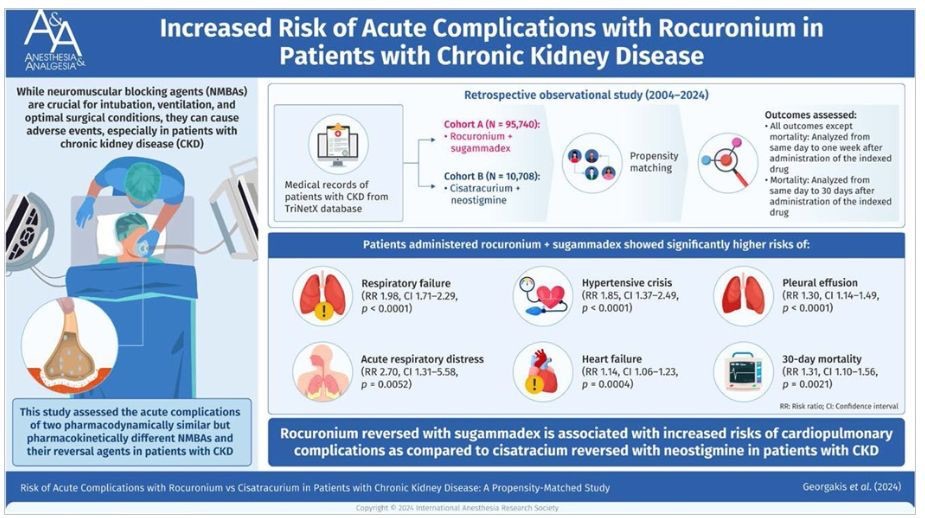
Rocuronium and CKD Posted on May 5, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...
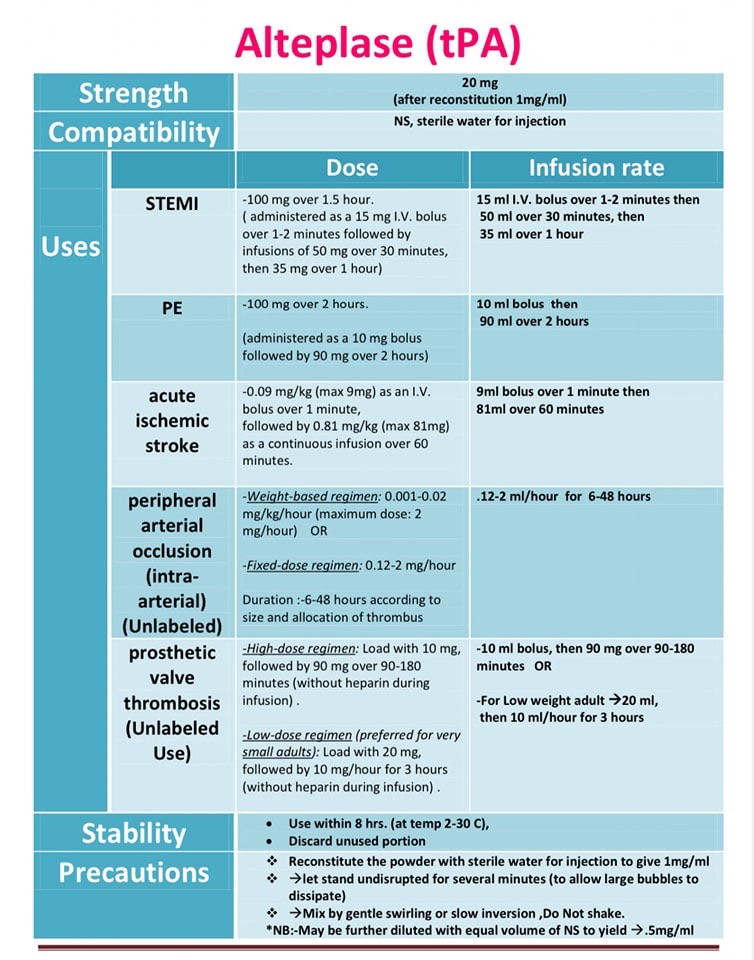
Alteplase Posted on May 2, 2025 by Dr Unnikrishnan Prathapadas Share this: Share on Facebook (Opens in new window) Facebook Share on X (Opens in new window) X Share on Telegram (Opens in new window) Telegram Share on WhatsApp (Opens in new window) WhatsApp Share on LinkedIn (Opens in new window) LinkedIn Email a link to a friend (Opens in new window) Email Like Loading...